Retroverted Uterus AKA Tipped Uterus
In my practice, I see many women who suffer from a retroverted uterus. A retroverted uterus is when the uterus is tilted back toward the rectum. A retroflexed uterus is when the uterus is flexed backward, kind of like a backbend. “The most common condition in women over the age of 50 is retroversion combined with retroflexion, in which both the cervix and the uterus swing backward, and the cervix lies on the rectum. At the same time, the small intestine lies on the bladder, pushing it down” (Source 1). Unfortunately, I didn’t know how to correct a retroverted uterus back when my mom had one. She suffered from horrible low back pain when she was pregnant with my little brother due to a retroverted uterus. She also suffered from terrible PMS, and I’m sure it was related to her uterine position. When the uterus is not in the optimal position, it restricts the flow of lymph and blood. Ovarian varicosities can result and lead to a disturbance in the communication between the ovaries and the hypothalamus of the brain, resulting in less than optimal levels of estrogen and/or progesterone. Restriction in the flow of lymph allows pathological debris to accumulate, causing acidity, pain, swelling, and inflammation. It’s like what would happen if the garbage collector and police officers in your district went on strike: garbage builds up, and mayhem ensues.
Women tell me all the time that their Ob-Gyn said that it’s normal to have retroverted or retroflexed uterus and that it doesn’t cause any problems, yet in the Obstetrics and Gynecology textbook, it states that “The retroverted, retroflexed uterus has three particular clinical associations: (1) it is especially difficult to estimate gestational age by bimanual examination, (2) it is associated with dyspareunia and dysmenorrhea, and (3) its position behind and below the sacral promontory may lead to the obstetric complication of uterine inculcation” (p. 12). “Estimation of gestational age in the late part of the first trimester may be difficult when the uterus is the RVRF or RV positions. The risk of uterine perforation during procedures such as dilation & curettage or insertion of an intrauterine device is increased in a woman with a retroflexed or anteflexed uterus. Applying traction on the cervix to pull the uterine canal into a straight line can greatly reduce this risk” (p. 37). There’s also a rare but serious condition called incarcerated uterus. Uterine incarceration is a complication whereby a growing retroverted uterus becomes wedged into the pelvis after the first trimester of pregnancy causing dyspareunia or urinary outflow obstruction. “Women presenting with urinary retention in the second trimester should have a pelvic examination performed to exclude uterine incarceration.” (4) Also, see source (6) below for more information.
“Recent data demonstrate that the prevalence of grade 2-4 uterine prolapse for a retroverted uterus is 4.5 times that for an anteverted uterus. Alternatively, 69% grade 2-4 uterine prolapse involves the retroverted uterus.” source (9) The retroverted uterus: ignored to date but core to prolapse
Another variation would be the anteverted/retroflexed (tipped forward but flexed back) uterus: a common consequence of cesarean delivery. In this study “an anteverted retroflexed uterine position was found in 27% of women after cesarean delivery.”
My mother had a hysterectomy and oophorectomy (removal of the ovaries) to treat her PMS and painful periods before she had a chance to go through menopause. I have to wonder about how this decision to have an oophorectomy at such a young age affected her brain. My mother was 38 years old when she had the hysterectomy. She was diagnosed with dementia at the age of 55 (although the signs started years before), and she died about seven years later. I found several studies making this connection between premenopausal oophorectomy and dementia.
“Premenopausal bilateral oophorectomy is associated with a higher risk, suggesting a dose effect of premature estrogen deficiency on dementia. The age-dependent effect suggests that the younger brain is probably more vulnerable to estrogen deficiency.”-Hysterectomy, Oophorectomy and Risk of Dementia: A Nationwide Historical Cohort Study (Source 1)
“Both unilateral and bilateral oophorectomy preceding the onset of menopause are associated with an increased risk of cognitive impairment or dementia. The effect is age-dependent and suggests a critical age window for neuroprotection.”- Increased risk of cognitive impairment or dementia in women who underwent oophorectomy before menopause (Source 2)
“Laboratory studies have shown that estrogen receptors are present on cholinergic neurons and have neurotropic, antioxidant, and anti-inflammatory effects. Estrogen deficiency in middle age has been postulated to account, at least in part, for the somewhat higher incidence of AD [Alzheimer’s Disease] in women than men and may constitute a risk factor for AD.”….the incidence of dementia or mild cognitive impairment is approximately 33% higher in the women with hysterectomy than in those women with a uterus regardless of treatment with hormone therapy or placebo”-Estrogen and Demential Insights From Women’s Health Initiative Memory Study (Source 3)

retroverted and retroflexed uterus AKA tipped uterus
Possible factors contributing to a retroverted uterus
- Severe falls to the sacrum
- Pelvic infection and inflammation aren’t really a cause but can keep the uterus in a malposition
- Uterine scarring from infections like Chlamydia
- Chronically poor pelvic alignment from wearing high heels, and sitting on the sacrum
- Endometriosis adhesions in the rectouterine pouch
Signs and symptoms of a retroverted or retroflexed uterus may be one or all of these symptoms. Please note that there can be other causes of the following symptoms.
- Painful periods
- Low back pain before and during your period. A heavy anteverted uterus can also cause back pain.
- Thin stools or constipation right before your period. The uterus significantly grows in volume before menses. (source) And can be even heavier when fibroids or adenomyosis is present.
- Foul-smelling menses. This is a theory and based on anecdotal evidence.
- Fertility challenges (5)
- Ovarian cysts
- Painful intercourse
- Ovulation Pain
- Sciatica (esp. with enlarged uterus, endometriosis or fibroids) (7)
- Prolapsed uterus (9)
If a woman with a retroverted uterus is able to get pregnant, she may suffer from low back pain and constipation until the adhesions holding the uterus to the posterior wall break free under the increasing weight of the uterus. This usually happens around 14 weeks into the pregnancy when the uterus gets heavier. The woman may experience back pain at this time and feel the uterus shift forward when the adhesions tear. This varies with different women depending on how long the uterus has been tilted back. By the way, the uterus does naturally move forward and back slightly as the bladder and rectum fill, but when the uterus remains stuck in any one position it affects the surrounding blood vessels and organs (bladder and rectum), as well as the health of the uterus and ovaries. Retroversion/retroflexion may make it difficult for the follicle to burst through the ovarian wall resulting in ovarian cysts. As for the ovulation pain, the ovaries sit very close to the psoas muscles especially when the uterus is tipped back and the psoas is already tight, this can affect the genitofemoral nerve causing pain in the front of the thigh and the knee.
I have seen a uterus adhered to the rectum in a cadaver. The person performing the dissection was able to break the adhesions between the uterus and rectum with his fingers. In a case as severe as that one, I honestly can’t imagine the manual therapies correcting a retroversion however, it should help with symptoms.
My approach to correcting retroverted uteri
involves softening, allowing, and encouraging rather than forcing. Forcing can lead to more adhesions. After softening the abdominal layers with gentle abdominal massage. I perform an Ayurvedic hip massage. Ayurvedic hip massage is the favorite part of the treatment for many women. From a manual therapy perspective, the hip massage helps to release muscular tension around the SI joint. The massage also brings fresh blood flow to the uterus, ovaries, and intestines. I will then apply specific sacral techniques rooted in the Maya tradition to encourage the uterus to move forward. It usually takes one to four sessions to get the uterus to move into the optimal position depending on how long the uterus has been retroverted. There are times, as mentioned above, that the position can’t be corrected manually due to strong adhesions or scar tissue. Even if the uterus can’t be coaxed out of retroversion, the massage can still help decrease symptoms by aiding blood and lymphatic flow.
I also teach self-care massage and movement techniques for retroverted uteri in my online Womb Care course.
Seeing a Nutritious Movement™ certified restorative exercise specialist for pelvic alignment may also be a good idea. The uterus attaches to the inside of the pelvis and sacrum via uterine ligaments, so if the pelvis is out of alignment the uterine ligaments won’t be loaded correctly leading to fibrosis. A posteriorly tilted pelvis also creates more intra-abdominal pressure on the reproductive organs.
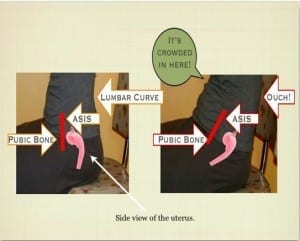
how you sit can contribute to a retroverted uterus.
Obviously, your pelvis should be able to move in many planes without causing organ dysfunction, the problem is the frequency of one position. When you sit, sit with your ASIS and pubic bone in vertical alignment. If you have trouble sitting with a neutral pelvis or feel like you’re forcing yourself into this position, you need to release the muscles that are keeping your pelvis in a post tilt. How you get there matters. You wouldn’t want to force a position. So, transition to zero drop shoes slowly to give your tissues time to adapt. Read more about elevated heels, pelvic position, and uterine position HERE.
I wish I could have helped my mom when she was suffering from the symptoms of a retroverted uterus. The fact that I didn’t have the knowledge to help her way back when makes me very passionate about wanting to help other women who have displaced uteri.
Update: I have been studying Visceral Manipulation™ (VM) since 2011. Visceral Manipulation™ is low force osteopathic techniques. To date, I’ve completed VM 1-6. Practitioners who have completed VM3 have learned techniques for freeing up the uterine, ovarian, fallopian tube, and bladder restrictions. In my private practice, I may use the retroverted uterus techniques I personally learned from Dr. Rosita Arvigo as well as Chi Nei Tsang (Chinese abdominal massage), Visceral Manipulation™, Ayurvedic hip massage and restorative exercise depending on the individual.
Update 2022: I recently received a call from an investigator at a California Sheriff’s department asking me if it was normal for a massage therapist to STIMULATE THE CLITORIS in order to correct uterine position. The answer is NO it’s not! That’s sexual assault. Apparently there have been several reports of a male massage therapist performing intra vaginal work and stimulating the clitoris of clients, claiming it will help correct uterine position.
It’s not uncommon for victims of sexual abuse to freeze or not speak up at the time of violation due to being in shock or doubting themselves about what they think is happening. It’s just too scary to comprehend in the moment. Plus, the abuser may use certain statements or medical terms to justify what he’s doing. I understand that it can be confusing as a client or patient when putting your trust in someone who is supposed to be an authority. Please know that it is in your right to say “no, that’s not ok” even if you can’t make sense of what exactly is going on. Your body knows! Trust yourself first.
Source 1 Hysterectomy, Oophorectomy and Risk of Dementia: A Nationwide Historical Cohort Study from Dementia and Geriatric Cognitive Disorders
Source 2 Increased risk of cognitive impairment or dementia in women who underwent oophorectomy before menopause from the Neurology– The most widely read and highly cited peer-reviewed neurology journal
Source 3 Estrogen and Demential Insights From Women’s Health Initiative Memory Study from the Journal of the American Medical Association (JAMA)
Source 4 The incarcerated gravid uterus: complications and lessons learned Obstetrics and Gynecology. 2014 Feb;123(2 Pt 2 Suppl 2):423-7. doi: 10.1097/AOG.0000000000000102
Source 5 Clinical variables affecting the pregnancy rate of intracervical insemination using cryopreserved donor spermatozoa: a retrospective study in china.International Journal of Fertility & Sterility. 2012 Oct;6(3):179-84. Epub 2012 Dec 17.
Source 6 Sonographic and Magnetic Resonance Imaging Findings in Uterine Incarceration
Source 7 Sciatica in the female patient: anatomical considerations, aetiology and review of the literature
Source 8 Uterine size measured by ultrasound during the menstrual cycle.
Source 9 The retroverted uterus: ignored to date but core to prolapse




This is so great!!! I’m a MATP too and this was very informative for me as well as my clients. I’d like to link it on my website, if that’s ok with you?
Absolutely. Sorry it took me so long to reply, your message was buried in SPAM.
Do you know anything about correcting a retroverted uterus with an IUD? Can the Arvigo work still be performed?
It definitely “flipped” forward around 5 months of pregnancy, but I had intense back labor with both babies (natural, midwife-assisted, thank goodness for the tub!).
However, when not pregnant, the biggest symptom I have is actually painful intercourse, since the cervix gets bumped directly. Not fun.
Thanks!
I wouldn’t attempt to correct a retroverted uterus with an IUD. I wouldn’t do any uterine manipulation with an IUD.
Are you sure it’s still retroverted? When the uterus is low the cervix may get bumped during intercourse.
Does retroverted uterus cause lower back pain? And do you see any symptoms of retroverted uterus in you early years? What precautions should a woman with a retroverted uterus be taking during pregnancy?
Edward, yes a retroverted uterus can cause low back pain, but not always. There are different degrees of retroversion.
Ideally, a retro uterus is corrected before pregnancy. As far as precautions, that is for her doctor to advise. Personally I don’t know of any. The uterus usually self corrects when the baby gets heavy enough.
How can someone do massage for retroverted uterus to reposition itself since there is no pratitioner in my area pls advice me
Hi Elizabeth, I can teach you the self-care massage via Skype. It is possible to correct it on your own depending on how long it has been retroverted.
Thanks again in your case
I had a retroflexed uterus with my last pregnancy. My baby is now four months old. Does the uterus automatically return to its prepregnancy position? I’m just wondering if my uterus is back to being retroflexed again.
The uterus usually corrects itself at five months pregnancy. It depends on why it was retroflexed in the first place whether it will go back to retroflexion again. If it was due to poor alignment of your pelvis (posterior tilted pelvis) and habits of sitting back on your sacrum and you are still doing that it may go back to retro again. I would do your self-care Maya massage (learn from a certified instructor) and do the “Down There” dvd as well as looking at your habits of how you carry your pelvis to prevent the uterus from going back. BTW, alignment of the pelvis is a whole body issue starting from the feet and working up. It’s too much to go into here, check out my site for alignment related posts and the Aligned and Well site. Find a RES in your area and if there isn’t one, I do SKYPE appointments and can look at your alignment and guide you.
Hi. I just found out I have a retroverted uterus when I had my first pregnancy ultrasound. I have always had SI joint pain and discomfort. It seems to be slightly worse recently. Any good pointers for exercises/moves I can do while pregnant? I’m only 11 weeks, hopefully I don’t have to wait for the promising 5 months where it may get better!! Also I am having a hard time finding an RES in Indianapolis. Do you have any resources or websites that may help guide me to someone?
Thanks!!
Hi Caitlin, Do you have the “Down There, For Women dvd? I would start there. And search the Aligned and Well blog for pregnancy posts, here is one http://www.alignedandwell.com/katysays/pregnancy-and-pain/
Did you search for a RES here,http://www.restorativeexercise.com/our-program-graduates/
If you can’t find someone in your area, I do Skype appointments.
I would like to learn the exercises to correct the uterus myself. I would like to get pregnant. How can I learn them?
Thanks!!
Hello, Thank you for contacting me. If you read towards the bottom of the post you will find links to find ATMAT and RES practitioners in your area, and a link to the “Down There” DVD. If you don’t find a practitioner in your area, I do Skype appointments and can teach you the Self-Care Maya massage for retroversions and the Restorative Exercises™.
Hello.
I have been suffering with constipation for most of my life. The most recent bout has prompted my doctor to do a CT enterography of my abdomen and pelvis. There is no bowel obstruction however the conclusion indicated that “the uterus is retroverted. The distal sigmoid colon is positioned between the uterine fundus and sacrum”. I have had 3 pregnancies.
Can you advise if this is something you have seen before?
Thank you
Becky
Hello Becky,
Yes, constipation can be caused by a retroverted uterus especially before your period when your uterus is heavier. I have seen this many times. If you were my client I would first correct the position of your uterus using ATMAT, and work with restoring motility to your colon using visceral manipulation. I may also incorporate pelvic alignment to ensure the uterus stays in the proper position and to reduce tension in the pelvic floor.
If you are not in Portland, I can teach you the uterine massage and pelvic alignment via Skype. I would first check to see if a certified ATMAT practitioner, and/or Visceral Manipulation therapist who has completed at least VM3 is in your area.
Best of luck to you.
Retroverted uterus trouble me a lot! I’m so glad to came across this article!!!!!!
Dear Barbara, my gynecologist told me that i have a retroverted uterus. I have had all sorts of issues from pelvic floor pain and other kinds of pains. I would like to know if there is anyway i can have skype lessons with you to collect my situation. I am glad to know that there is someone like you who can help a lot of women with the same condition i have.
Hi Nickita,
If you do not have a certified ATMAT practitioner in your area, I would be happy to teach you through Skype the Maya massage to correct uterine position. All the details for making and preparing for your appointment can be found here,https://alignmentmonkey.nurturance.net/2011/now-offering-skype-appointments
I m 22yrs old ..got married before 1 nd half year..I hav problem of scanty menses ,pcod of both ovaries and retroverted uterus..please guide me
Hello Ambar,
Did you read through the article? I do have links and recommendations in the article.
As for PCOS, getting your blood sugar under control is extremely important as well as reducing stress (when cortisol goes up, so does insulin). PCOS is insulin resistance in the ovaries. The herb formula Sweet Blood is traditionally used with Female tonic for PCOS. I make both the formulas and can give you more information if you are interested.
Hi, I have a retroflexed uterus, im 30 (not pregnant) one child age 10.and for approx ten yrs now I have sciatica pain, gets worse with periods, pain down my leg. Not stomach pain just gurgling noises.but the leg pain,is unbearable.I also get the usual diahorrea headaches, n embarrassingly smelly farts.docs say the uterus has nothing to do with my sciatica, nor does my l1 compression fracture..could I have ur opinion please. At the wits end
PS been checked for endo, cysts etc all clear
A retroflexed uterus can cause venous congestion that gets worse right before or during menses. Cases of atypical sciatica can be caused from venous congestion of the epidural veins that in turn irritate the sciatic nerve roots. The first step for you would be to correct the position of your uterus by seeing a certified ATMAT practitioner. As far as the headaches and diarrhea go, it may be hormonal. Sometimes ATMAT and vaginal steams will also help balance the hormones once hemodynamics is restored. Diet and herbal therapies may also be recommended by your ATMAT practitioner, ND, or other health care provider.
THIS is the greatest article I have read in a long time! Thank you SO much. Love your site and all your amazing info! I share much of it with my students and will be posting a link to this article on my website and facebook pages.
I am so terribly sorry about your mom. 🙁 My heart goes out to you. She would be so proud of you. I remember when pretty much every young women would up having a full hysterectomy. it’s a crime and I had no idea about the dementia link. I find this so frightening yet fascinating. I have also contacted a practitioner in my city and am hoping to hear back from her. I’ll keep you posted on my results! Thank YOU!
Thank you so much for your kind words Lori.
Yes, please keep me posted on your results. Make sure you see someone who has been certified. The retroversion techniques aren’t taught until certification week with Dr Arvigo.
How can you tell if you have a retroverted uterus? The symptoms fit. I have not had a child. At 47, I menopaused and a few months ago, something shifted so my perineum is up and my rectum seems odd–slightly numb and . I get pain around the tailbone. I’ve had a colonoscopy and a CT scan to look for tumors. My gynecologist performed an ultrasound. We were not looking for an inverted uterus, though.
Either from the symptoms, or from an internal exam. An ATMAT practitioner will also do posterior work on your tailbone and pudendal nerve. A pelvic floor PT should also be able to help you with that.
When estrogen declines as a woman goes into menopause, old injuries can surface causing pain around the site.
I just wanted to say THANK YOU for writing this article! I’m going to be meeting with an Arvigo practitioner in my area. I’m so excited.
Wow alignment monkey we must have some cyberspace cosmic connection I was googling for some information on a retroverted uterus and I came across your site again! I wish you were in my area!
I have only just realized this and am a bit puzzled? I have been having weird sensations as if something is moving around “down there” since a while when I saw a gynecologist she examined me and on the letter said I had an anteverted uterus but then on the report from an ultrasound a few weeks later it says it is retroverted! The gynae never mentioned it on my second visit and I have only just noticed it on the letter. In your experience / research is it common for the uterus to move like that, surely its relevant and she should have mentioned it to me? Im in my 30s not pregnant or ever had a baby. I suspect I may have endemtriosis which might be something to do with it?
Hi Lulu,
Yes the uterus can and does move around. It’s position can be influenced by bladder and bowel fullness, and prolapsing intestines as well as pelvic position. The movement influenced by the bowel or bladder should be minor though. Were you closer to starting your period during the the ultrasound? Perhaps the weight of the uterus contributed to the uterus falling posteriorly. Did they place your pelvis in a tilted position to do one exam, but not the other? If they are diagnosing extreme variations as you have noted, I’d suspect uterine mal-position due to poor pelvic alignment and lack of strength in the ligaments. Endometriosis can contribute to poor uterine alignment through adhesions and on the flip side, a retroverted uterus can contribute to endometriosis. It is my experience that combining ATMAT and Restorative Exercise™ can keep the uterus in her natural position while allowing for her natural mobility/motility.
Hi…my uterus is shifted to the right. I believe this is the cause for my painful periods and clots. Do you know the messages to correct this?
Yes, an Arvigo Techniques of Maya Abdominal Therapy™ practitioner can reposition a right leaning uterus.
Thank you! Is it something you can show me how to do via Skype? I don’t have a certified therapist close enough to where I live.
Hi Karina, I’m sorry, but I can’t show you the retro techniques via Skype. The retro techniques are a bit more complicated and can’t be done on oneself. I can teach you pelvic alignment via Skype which is crucial for correcting retroversions.
I am so glad I found this! I am 10 weeks pregnant and I have a retroverted uterus. I have been having severe constipation and abdominal swelling despite ample fiber, water, clean diet, and stool softeners. My stools have been narrow and I think this is related to my uterine position. Is there any hope for relief or things I can do? I would be interested in Skype appointment because there are no practitioners in Kansas
Hi Emily,
I’d be happy to do a SKYPE session with you to help with pelvic alignment. This is the first step to correcting uterine alignment at your stage of pregnancy. The uterus may self correct when the uterus gets heavy enough to fall forward, usually around 5 months along. It can correct earlier with pelvic alignment work.
I have RV uterus & also diabetic pt.I have no children.may i pregnant through these disease?
retroverted uterus is not a disease and you can get pregnant with a RV uterus, but it’s more difficult to become pregnant and one may suffer from constipation and back pain as well as increased chance of miscarriage. It’s best to correct the position before getting pregnant.
Barbara- I cannot thank you enough for this brilliant information!!!! For years I have suffered with unbeleiveably painful intercourse coupled with the most severe unexplainable UTIs that never ever go away. My doctors have all been baffled. I just figured my body was messed up and nothing could be done. Years ago during a routine pap my dr said my uterus was tilted- I didn’t think anything of it it was only until today that I read that tilted uterus can cause all of these issues!! My main questions for you are how long does it take to reposition the uterus, how long will it stay in the correct position, and will the severe uti’s and intercourse pain go away totally? I can’t tell you how excited I am to avoid surgery! God bless!
Also- my uterus has probably been tilted all my life- I am 30 and I can’t remember a time when I didn’t have these issues. Because this has been so long standing- will it still be fixable? Thanks!!
Great article. Thanks for your clarity and details of information, helpful for so many! I do both abdominal myofascial release work, Arvigo’s work, and internal integrative pelvic care/holistic pelvic care to help with retroverted uterus. An osteopathic physician friend says that restoring the cervix/uterus to center and neutral is of primary importance for women’s pelvic health, and the first thing they address (manually-internally) when dealing with any pelvic issues.
Let me start off by saying I have Crohn’s disease and MS & I am 35 yrs old. I have had several surgeries and finally had my colon removed 2 years ago. I have 2 children, both c-section. I had the essurance coils implanted for permanent birth control and was informed my uterus was tilted. The last six months I have been having horrible back pain, fowl smelling periods, and periods that last for 8-10 days. It is like it will drain, stop for a day and drain again. Horrible smell….. Well your article finally helps shed some light on what might be going on. A small part of my rectum was left when my colon was removed so it is totally possible my uterus it folded over it and causing this pain and odor. My question is where do I start with my doctors? My gastro? My Gyno? What are your thoughts? Thank you in advance for your help!
Yes, it is possible. I’m not familiar with the coils, but I don’t recommend the IUD,s with retroverted uteri.I would check with your gyno to make sure everything is OK with the coils. The uterine corrections can’t be applied with coils, IUD, mesh or other foreign devices present.
A (very delayed!) thank you so much for your detailed reply. I have looked and there are not any ATMAT anywhere near me, unfortunately its not the sort of thing I would trust a lot of physios or massage therapists with- I don’t want someone heavy handed poking my bits around lol! I have been doing the pelvic list trying to keep my feet straight, backing my hips up etc. Would you still recommend the down there DVD too? Thanks again.
Yes, I definitely recommend the Down There dvd, or a Restorative Exercise™ Skype appointment with me. Sometimes Restorative Exercise™ is enough to restore uterine position, but sometimes manual therapy from a certified ATMAT or Visceral Manipulation™ Therapist is required. Either way correcting pelvic position through Restorative Exercise™ is extremely important to uterine position. Try looking for a Visceral Manipulation™ therapist who has completed VM3 since you don’t have an ATMAT practitioner near you. You can search on the Barral Institute website. VM3 is not heavy handed, it’s very gentle osteopathic techniques.
Hello, I am happy to find this information. I am 30 with no pregnancies. I have had abnormal menses from the time they started. Extreme pain, heavy bleeding etc. My mother also had this. I have been on oral contraceptives to regulate my cycles for over 10 yrs.
A few yrs ago I was told I have a tilted uterus, no one seemed concerned. On and off during my sexually active yrs I have at times experienced abnormal bleeding, extreme cramping during and after sex.
I have been skipping my periods with the advice of my GYN bc during them I experience a fibromyalgia flare up. It takes weeks for me to feel better, then when I do it is time for another period.
I skipped it for about 6 months most recently. Most recently I have felt pain during and after sex more often, also having a feeling of menstrual cramps randomly throughout my day. I thought my body may be trying to have a period, so I had one. Moderate-heavy bleeding, cramps and a fibro flare up.
I told my GYN my concern about my pain on/off. My 1st cousin on my maternal side has a history of endometriosis. My GYN most recently sent me for a pelvic and transvaginal ultrasound- the test showed no reasons for pain, such as endometriosis. The technician did mention my tilted uterus in relation to how she had to move the probe internally.
Since the ultrasound provided no other information my GYN sent me for a consultation for a laproscopy. I am reluctant to have this as it is a surgery, the DR did say I could try to medically manage without laproscopy. I am reluctant to treat something unless I know I have a condition.
The DR did remark that the fact I have been on an oral contraceptive all these yrs, he is not highly suspecting alot of endometrial scarring. During my visit I was asked about any STI’s in my history.
I had contracted chlamydia 6 yrs ago from a cheating boyfriend. After diagnosis I estimated that I had it for about 7 months. Had treatment and resolved the infection, during consultation the DR did say that could have caused scarring too.
I realize this is alot of information. I felt I had to ask what opinions you may have on my situation bc the information I found on this posting made me wonder if the position of my uterus could be to blame, and is it possible to be tilted without endometriosis or other scarring being the culprit.
Hi Joanna,
Yes, it’s possible to have a tilted uterus without having endometriosis. Next time you talk to your GYN, ask which way it is tilted. They wouldn’t be able to diagnose endometriosis with ultrasound. If it were me I would try correcting my uterine position with ATMAT and doing Restorative Exercise for pelvic alignment. When the uterus is out of alignment, blood, lymph, nerve and energy flow will be impeded and pain and dysfunction will result. ATMAT won’t change scaring within the uterus, but it may help reduce your symptoms.
I’m glad I found your site!thanks
I got tilted uterus since 2006. Due to lifting my baggage!
In my country, Indonesia, there are massage therapists that can fix uterus to it proper place.My family knew one since 30s years ago (she’s 76 yo and still giving therapy).
There are people who said they can do it, but you must careful. This granny is great! she even can fix a lady uterus that already has rings and some of her inner is out of her body to proper place.
Oh yeah my sister got pregnant after 11 years marriage with her help too.. (and some many women…)
So since 2006 I keep going to her regularly (usually 1x a month) and I always use core strengthener whenever I travel.Anyway I keep got tilted and sometime it really bad (I got fever for days). Though I have very regular period without pain & she said I got good fertility. If I got mild tilted uterus, I just do a headstand so it will go back to proper place.
But I will leave my country to go to Europe for long time.I’m sure I will get tilted again cos I’ll travel and I wonder where can I got this uterus problem fixed when it occurs.
I ask my therapist if the massage can be done without her.She said it can, but I dunno if she can teach since she need lots of rest now due to just recover from an ill.
So I’m really glad that there is a similar massage out there from other nation = maya abdominal therapy. and it has self care class. I’ve also found the practitioners/teacher in Europe. So I don’t need to worry about my uterus issue! Thanks a lots.
That’s great that you have a granny healer that can help you and other women in your area. We have so much to learn from our elders! I have so much appreciation in my heart for their teachings.
Hi I am 22 years old and I suffered a miscarriage back in april I was 15 weeks pregnant. I had to have a D n C performed. I didnt get my first period until june and its so painful its shorter now but its super heavy flow. And last week I went to the emergency room because I had terrible back pain and all they said was I had a retroverted uterus. I didn’t know what it was til I did the research. Do you think its a good idea to go get a massage to get it fixed which the lady said “you’ll get pregnant right away” ?
So sorry for your loss. Yes, I would see a certified ATMAT practitioner to correct the position of the uterus before trying to conceive again.
I’m so glad to have stumbled across this site.
I’m 25 and recently found out that I have a retroflexed uterus. I have always had heavy bleeding and extreme lower back pain during periods esp on my right side, as well as runny stools before my period and constipation during.
I was told that it shouldn’t affect my chances of becoming pregnant, however your site states that it may cause “fertility challenges”. I was wondering what type of challenges i.e. falling pregnant or increased risk of miscarriages?
Is it important to try and fix a retroflexed uterus before falling pregnant even though it’s expected to become anteverted with the heavy baby?
Hello Mary,
Yes I would correct your uterine position before conceiving. I would give yourself three months at least before trying to conceive once you start ATMAT treatments so your body has time to make corrections, cleanse and rebuild a healthy uterine lining. The retroversion may make fertility a challenge, increase chances of miscarriage, and make pregnancy uncomfortable (constipation,backache, hemorrhoids).
could you please help me by sending me the natural solution for my Retroverted Uterus
Your article answers so many questions of symptoms I’ve experienced for years! I wish docs would explain a tilted uterus when they tell you that you have one. I’ve read so many times now that a retroverted uterus corrects itself during pregnancy around 12 weeks or so. I am hearing you say around five months. You say it tears from where the adhesion is but what will that feel like? How long will that pain last? Will the mother feel more fetal movement after this happens? Is it common to feel the baby really low near the cervix before feeling around your belly due to the retroverted uterus?
Thank you so much!
hello, I just went today to my gyn and she said that my uterus moved all the way to the right side.
what can I do to move it to the right place?
thank you
An ATMAT practitioner can correct a right leaning uterus and teach you the self-care to make sure it stays in the optimal position.
Hi Lindsay,
On average 4 to 5 months, but I’m sure it varies depending on how long and to what degree your uterus is retroverted. Some women say it is a sudden pain that doesn’t last but a moment, others say there is no pain when it corrects.
I would say the answers to your other questions would be “it depends”. Those would be good questions for your midwife or OB/GYN, they can access your specific situation.
Hi Sharon, I’ve outlined the steps in the article. If you mean, how to do the ATMAT, you would have to learn self-care techniques from a certified practitioner. Sorry, it’s too complicated to explain and the retroversion techniques are done by a skilled practitioner.
HELLO,
THIS IS MY FIRST TIME KNOWING ABOUT THE TILTED UTERUS all the way to the right, can you please tell me what can work for me? and the maya abdominal massage works?
and one more question: how long do you think it will take to align my uterus.
thank you for your help.
I don’t know what you mean to teach me the self care, the self care what?
The self-care is a specific abdominal massage taught by an ATMAT practitioner. I also include pelvic alignment exercises in the self-care.
Yes, the Arvigo Techniques of Maya Abdominal Therapy™ is very effective in correcting a right leaning uterus. I would say on average it takes 1-3 months to correct the position, depending on what is specifically going on with you, your pelvic alignment and if you are consistent with your self-care massage. Also read my post: https://alignmentmonkey.nurturance.net/2013/can-the-uterus-be-trained
It may take 1-4 professional sessions. When the uterus is leaning to the side, it is fairly easy to correct, depending on existing adhesions.
Hi Barbara, thxs for this information. I m 30 yrs old. During ultrasound I come to know my uterus is retroverted. I don’t feel any pains during period and also no back pain. I currently got miscarriage of 4 weeks. Is this responsible due to retroverted uterus?? How can it be treated?? Thx u..
I’ve noticed that about a week before I get my period, my lower back would hurt. I’ve always had low back pain as long as I can remember. I thought it was due to an injury. However I’ve been living more holistically. I usually get chiropractic adjustments and massage therapy. I’ve had a feeling lately that my low back pain was caused by my uterus but I just do yoga, get adjusted and move on. The last few years my periods been extremely heavy, so heavy I would have to change pads every hour or so. That would be day 3. Now that I’m 44 it’s still heavy, but after day 3, I’m done. I’ve seen my ob/gyn, had an ultrasound due to another condition, and everything looks normal. But it isn’t. That being said, I acted on my awareness today and came across this blog. Thank you. There are practitioners in my area and will contact one today.
Hello, I really enjoyed reading your article. I have a retroverted uterus. About a year and a half ago I had an oopherectomy on my right side because of a baseball sized dermoid cyst that had completely taken over my ovary. The Dr’s said there was no ovary left. With a retroverted uterus is it normal to have a very low cervix? My OBGYN has never said anything to me about having a prolapse, but while reading Take Charge of Your Own Fertility I found that my cervix is very near the opening of my vagina. I find this extremely strange as I almost never have pain during intercourse. I am scheduled to receive treatment with an acupuncturist and Mayan massage for fertility soon, but have been concerned about my findings with my cervix. Thanks for the great information here.
As a rule, I wouldn’t say retroversion and prolapse go hand and hand, but I can see how there could be a relationship. Maybe your OBGYN didn’t notice the prolapse because you were supine and didn’t have gravity working against you. And perhaps your exam was during a time in your cycle where your cervix was higher.
Wonderful that you are getting acupuncture and Maya massage, they work well together. Make sure you mention the prolapse to both of them-there are specific techniques they both can do for prolapse and for retroversion. Best of luck to you.
Wow. It’s amazing how I’d accepted the fact that cysts and a gauntlet of misery and pain were normal simply because there was nothing I could do. I lead a pretty natural lifestyle, minus the week I am on my period and then I become a pill popping ball of shame. I’ve had to have a steady narcotic grade prescription for the pain for as long as I can remember. I know this can’t be good on my body, but I’d tried literally everything – and even with the medication I have to use a combination of other tricks. I’m only 24 and now am having so many issues that drove me to the internet to see if, in fact, there was something that could be done. THANK YOU THANK YOU THANK YOU for posting this. Unfortunately I don’t have any practitioners in my area, but at least now I know there’s hope! 🙂 Thank you!
I am 59 years old and I believe I have a tipped uterus. There is no pain, no back pain, and no issues with our sex life. Now, I DO need to lose @ 40 pounds! I rarely go to the doctor, but I am wondering if I need to get something done about this. Any exercises other than the ‘posture alignment’ exercises?
Hi:
I just went to the OBGYN ( I’m 31 years old) and my whole life have not enjoyed sex due to pain during intercourse. I’ve mentioned this to many OBGYN and they never seemed to be helpful. Today during my appt I mentioned it and when she was examining me she said oh you have a tilted uterus…that’s all she said. I said what? Is there something I can do to alleviate the pain. She said “you can try to angle him further down during intercourse it’s not a big deal 1 in 5 women have it.” but to me this is a big deal because it’s affecting my marriage now because I don’t want to have intercourse due to the pain. She did not ask me to get an ultrasound or anything. I came home and starting researching and came across your site which was so helpful. I was wondering if you know the success rate with treating a tilted uterus? Is this something I should get an ultra sound for to learn the exact position? How much would something like this cost to fix?
Hi Dana, Look up a certified Arvigo Therapist in your area at http://www.arvigotherapy.com. Make sure the practitioner is certified because Dr Arvigo doesn’t teach the retroversion techniques until the certification level. You don’t need an ultra sound to find the position of your uterus. I would call and ask your OBGYN which way your uterus is tipped, she probably recorded it in her notes (anteflexed, retroflexed, left leaning, right leaning, retroverted, etc). If she can’t tell you, your Arvigo practitioner should be able to tell by palpating your lower belly and by your specific symptoms. On average it takes 1 to 4 treatments over the course of three months to get the uterus to stay in it’s ideal position. It all depends on how long it has been tipped, how often you do your self-care massage and in some cases changing pelvic alignment and shoe choice. I suggest the “Down There” DVD as a starting place for pelvic alignment. The cost for the treatments on average is $120 for the initial 90 minute appointment and $85 for 60 minute follow ups. Correcting a tipped uterus is not difficult, but could be challenging or not possible using manual techniques if it has been tipped for many years and adhesions have formed due to inflammation from infection, or scar tissue from surgery.
Good luck! Let me know how it goes once you receive a session.
Hi Barbara,
I came across your website whilst searching for information about a retroverted uterus and rectum heaviness sensation.
I am 38 yrs old and have had 4 children. I have a frontal vaginal prolaspe and minor rectal prolaspe, that has improved with Yoga and physiotherapy. Despite the work I have already done, I still get this heavy feeling every month at ovulation and before my period. I have often wondered if my retroverted uterus is placing pressure on my rectum. I have had many internal scans of the uterus and all looks ok, except for minor thickening in one area and free fluid in the back of the uterus. Have you heard of similar?
I am in Australia and I don’t believe there would be any practitioners here.
Hi. I would like to discuss my case with you for some possible suggestions. How can we connect via Skype?
Mine is a question I’ve had for awhile. I’m hoping for a reply. I was told I had a retroverted uterus many years ago. Since I can remember my periods always caused a day or two that I have to stay home. It is like all of the blood is realeased at once. I soak two super tampons every 10 to 15 minutes while it is going on. The heavy bleeding last about 24 hours. I buy two 40 count boxes of super tampons and pads and use them all up during the 24 hours. During and after this I feel dizzy, clammy, and have a horrible headache. I find it hard to stand with out feeling unbalanced. Much of the time the tampons don’t work and I have to stay in the shower and mash on my tummy to help the large clots come. My question is could the tipped uterus be causing my period blood to be held back in the beginning and then just come out all at once when it becomes so full and heavy. Thank you in advance.
Hi Rebekah,
I too am in Australia (QLD) and have stumbled across this site after ‘fishing’ for information.
A became aware of my tilted uterus in 2012 after an ultrasound I had trying to get to the bottom of 5 months without a period. I didn’t ask for any details as I was told this was normal.
A short time after that ultrasound I got my period which lasted 4 weeks, I lost about 2-2.5 litres of blood in that time and became very anaemic (as you’d expect).
Since that time my periods have been very heavy. The relationship I connected to this was that I had given up the contraceptive pill late 2011 and my body had finally adjusted to that.
Jump forward to the end of 2013 and my periods became crazy heavy, I had 2 periods that lasted a little over 2 weeks each since just before Christmas last year, had me in all sorts of pain and unable to do anything that required any distance between me and a toilet. I am again anaemic as you would expect. I have recently had another ultrasound (I don’t like scans at all… but no idea how to avoid it), they also had trouble scanning due to the tilted uterus (again I didn’t ask for specifics) but did comment that based on my lining seen at the time, I could expect yet another excessive blood loss when my next period comes around. That was about 5 weeks ago.
I recently moved from SA to QLD and have had to change chiropractors (which I have been seeing for several years). I have always preferred a holistic practitioner and have found one that interestingly has a special interest in organs. Anyway, I went through the usual Q&A mentioning the periods and hormonal inbalances that the doctors are constantly trying to put me on medication for… but can’t and wont take… and his first comment was “it sounds like your uterus may be tilted, I will check for that”. Let me make this clear, I didn’t tell him this in the Q&A because as far as I was told a tilted uterus means nothing.
So he did his thing and determined my uterus was tilted and he adjusted it. Now I am VERY open to alternate solutions but even I thought he was weird!!! That adjustment was 2 weeks ago.
Since then, I have been going to the loo regularly as I had been somewhat constipated which I knew but thought I must be eating poorly. I got my period a week ago, it has been and gone and was what was a typical flow for me before they became heavy in 2012. For the first time in almost 2 years I was able to go out whilst I had my period… not that I did, I was concerned it was the calm before the storm and that any moment I was going to start the flooding.
With all the reading I have done since these events it seems as though the tilted uterus may have impacted the natural progesterone levels allowing the estrogen to run riot which subsequently led to the periods I was experiencing…
I am REALLY sorry for this long response here… but I am still amazed by what has happened and all of this was to just say, my Chiropractor seemed to have adjusted mine.
FYI – when I look for a Chiropractor, they must also practice Applied Kineseology as they are gentle in comparison to the traditional practitioners and take a holistic approach to their clients.
Good luck… and again sorry for the long winded response. It’s the first time I have really communicated these results so I’m a little excited 🙂
Hi,
I realize this is much later in time than when you posted this, but I am thankful for the information. I was diagnosed with a severely retroflexed uterus during a d&c last Friday and my doctor seems to think that I have to just live with it. I know I wasn’t always this way, or at least didn’t always have the symptoms. At 6 weeks into the pregnancy, I had to take a ride in an ambulance and stayed 4 days in the hospital because I couldn’t walk. My OB thinks that the pregnancy did not affect the back pain. At. All. I know my body and disagree… So my question is that my PCP and OB seem to think that the uterus would go back after a manipulation no matter what. Do you have any resources or examples of how ATMAT and correct alignment can be a long term solution to a severely retroflexed uterus? (I have no endometriosis, fibroids or PID).
If the uterus is able to be manipulated back into position (no adhesions keeping it there), I don’t see why it wouldn’t stay, as long as the pelvic alignment is addressed as well. Have you read this post? https://alignmentmonkey.nurturance.net/2013/can-the-uterus-be-trained Click through to the interview. Andrea Muraskin had a retroverted uterus and was able to correct it with ATMAT. You can see the before, during and after self-care ultrasound photos at the end of her post. I spoke with her recently and she said that it’s no longer retroverted. And yes, a retroflexed uterus during pregnancy will cause back pain, as the baby and uterus grow it only makes sense the uterus will push into your back.
My retroverted uterus stayed in the ideal position after correcting it with ATMAT treatments and Restorative Exercises for pelvic alignment. If you remove the reasons why it went out of alignment in the first place, why wouldn’t it stay? That’s what I would ask your PCP and OB. I’d like to hear their answer, maybe I’m missing part of the story?
This was a very informative article, thank you! I have been to several OBGYN’s and they always tell me my cervix is tilted. However, they never say in which direction. They always get really low and dig around for it. I was reading through the symptoms and I would say I have most them. The regular lower back pain and painful intercourse are my most frequent symptoms. The doctors have never been too concerned with my tilted cervix. We have been trying to conceive for 6 years and I am wondering if this could be a factor? Who do I speak to about my concerns? Do I talk with my OBGYN or my Reproductive Endocrinologist?
Yes, a retroverted uterus can affect fertility. Ideally you should see an ATMAT practitioner trained in these techniques for hands-on therapy and a Restorative Exercise Specialist™ for pelvic alignment, both of which are important components for uterine health. Your OBGYN most likely won’t do anything to reposition your uterus.
See links above.
I’ve always had a tilted uterus. I found out in my twenties. I’m in my thirties now. Definitely explains the painful poops and the necessity of creative sexual positions. lol! Great article!
Hi I have a ‘very retroverted uterus’- scan with a mc showed this, had to have internal scan. I’ve got one child- 2yrs.
I have lower back pain around the tailbone and it hurts to stand up from sitting.
I have pain when ovulating- always know it’s happening- lasts 7 days ish. Hurts inside when I sit down during this time. Sex also feels tender during this time- not painful though.
I have experience small bleeds for a day or two at the start and end of ovulation? Have you ever known this?
Clear smear October 2013 but previous colposcopy and heat loop treatment in April 2013.
Realised reading this article too that my posture when sitting is awful ! 🙂
No bleed other than ovulation time. Been tracking it for 6 months. Keep goin to and for gp. No infections or anything either.
Yes, sometimes pain during ovulation can be a sign of displaced uterus. The ovaries get larger during ovulation and if they are irritating surrounding tissues like the psoas, you could get pain. The retroverted uterus can also cause disruption in blood, lymph, nerve and energy flow causing inflammation, discomfort and even hormonal imbalance. Sometimes the bleeding around ovulation can be about the sudden shift in hormones.
Thank you! Even though you have had a displaced uterus for some time, you still may be able to correct the position with ATMAT. Even if it has adhered out of place, ATMAT can help with blood, lymph, nerve and energy flow in and around the uterus.
Thankyou for a quick reply. I’m still goin back to gp but they don’t seem to know as much about this issue. Awaiting to see if I pregnant this month- if not I will look into massage to realign. Such a helpful sight.
During ovulation when bleed occurs, only spotting, it does worsen with a bowel movement?
Like I say I am goin back to gp- but my instinct is it’s linked to cervix/ uterus lying on rectum? Is this possible?
I’m going to request stool sample and full blood test. I do worry.
Yes, it’s possible that the cervix or uterus is lying on the rectum.
Hello,
I stumbled upon your site and very grateful that I did. I didn’t know a retroverted uterus could be fixed. When my gyno told me I had one, she just said it was normal with some women and on top of it I have multi “cluster” fibroids. I also am dealing with a pelvic problem where my pelvis was pushed out of alignment by a chiropractor where my right hip was over adjusted forward and under and my pubic bone is no tiled towards my right hip. I couldn’t sit straight for months and had to keep pushing my pelvis back, yet I have consistent shifting of my muscles and fascia in this area pulling the pelvis forward and preventing full stretching. It has shortened the muscles in the back of my legs and psoas. I stretch and do all of that, been trained in yoga, pilates and was a professional dancer. This has caused more pain and problems then needed as I already have fibroymyalgia. Do you have any tips for me and do you know of anyone that could help in the Toronto Canada area?
Thank you and Kind Regards.
It has been my experience that most retroversion can be corrected. There may be cases where too many adhesions have formed restricting the uterus from moving forward. Even if the uterus is adhered, ATMAT and RE can help with blood, lymph, nerve and energy flow and greatly reduce or eliminate symptoms. In your case pelvic position is extremely important to correct since it sounds like the primary cause of your uterine displacement. A certified ATMAT practitioner should be able to do some pelvic corrections in addition to the uterine work. I would also recommend a Restorative Exercise™ specialist, I know there are some in Toronto (check out http://www.restorativeexercise.com for a list of practitioners). The “Frankie Says Relax the Psoas”, “Hams and Quads”, “All Around the Thighs we go” and “All Fo’ The Pelvic Flo'” may be be good Alignment Snacks to get started with. (see Alignment Snack banner to the right). Looks like there is one certified ATMAT practitioner in Toronto: https://arvigotherapy.com/users/dr-verna-hunt-bsc-dc-nd
Hi Both my sister and I have retroverted uterus and we both have the same painful periods with the same symptoms, pain in colon, not able to sit, constipation, pms, ovulation pain… On top of it we have fibromyalgia episodes. And IBS. Plus when my soster got pregnant she could not bare it. We’re not twins but it’s probably genetics (my mom doesnt have it and noone on my moms family so its probably grandma…).
We have had the retroversion probably since birth.
Can these exercises work on genetics?… The uterus must bw attached that way?… Thank you SO MUCH.!!!
I believe my retroverted uterus is causing adrenal/ thyroid/ cortosol/ progesterone issues which is turning into auto immune issues and poor health despite geed dietary habits. I have been to an Mayan Abdominal therapy coach and natrapath but so far not seeing any changes 🙁
It is true that RVF is actually asymptomatic in most of the cases. If it is symptomatic, get the treatment which improve the symptoms.
The asymptomatic RVF is actually a mobile one, in whom she is not feeling any discomfort.
And by the way, why so early to do unnecessary hysterectomy at 38 years old?
Yes, the uterus can be retroverted and asymptomatic if it’s mobile. But I’ve also seen several mobile retroverted uteri cause symptoms, including in myself.
Back in the 80’s it was common to take the uterus out for the PMS and painful periods. One saying was CPU “chronic persistent uterus”, or “there’s no room in the tomb for the womb”. Basically, if you weren’t going to have more children, the uterus wasn’t serving a purpose and was seen as a potential place for cancer.
Sorry to hear Tania. Hormones and adrenal function can be complex and involve many factors (as you know). I wouldn’t think a retroverted uterus would be at the root of the problem. My first thought would be gut health (which it sounds like you’re probably working on with your ND). I know when it comes to adrenals, it’s a longer term process to correct. Best of luck, I hope you get some relief soon.
Hi, thank you so much for this information.. I am only 16 and going through all of the symptoms of a tipped uterus and I don’t know what to do at this age to help with it. Around my menstrual cycle, I have a LOT of pain and I get really constipated. And yes, I have been active and go through pain during intercourse as well. Is there any advice you could give me on what to do? I’m scared..
I found out recently that I have a retroverted uterus and also Adnomyosis. I have had 4 children two vaginally and the last two by c-section. The believe the Adnomyosis is from the c-sections and I’m wondering if it isn’t also causing the uterus to retrovert. Do you think that Arvigo can be done to at least put it back in the right position or would the Adnomyosis prevent it from moving?
Hi Sarah,
Whether the uterus can move out of a retroverted position depends on a number of factors. Mainly the degree of adhesions and your pelvic position. Either way, the Arvigo work will help the function and health of the organs by improving blood, lymph, and energy flow even if the uterine position doesn’t correct. I would also work on pelvic position, the “Down There” for women dvd is a good start. http://nurturance.net/content/store.php
I think that I may have a retroverted or retroflexed uterus and that it recently occurred or got worse. I had in the past noticed some pain during intercourse, but nothing to really pique my concern. Recently I became “constipated” but after all of the methods of trying to unblock myself were worked out, I realized that there was nothing blocking me up in my bowel, it was pressing from the outside! I had to use my own fingers to figure all of this out and a whole lot of reading, as doctors just dismiss you. My doctor is still convinced I have an impaction even though they can’t find one in any tests. Anyway, I don’t know how this could have come on all of a sudden or what to do about it. I’m so frustrated b/c I have to use a laxative to go to the bathroom even though I don’t really need a laxative, I just need my uterus out of the way! I’m always all backed up and feel terrible. I had an ultrasound, but the tech told me there was no way my insides were causing my back up and that I needed a colonoscopy. I’m overwhelmed. What is the best test to actually SEE the problem? Is it an MRI? I’ve scheduled a well woman exam now that I’ve figured out it’s not a bowel issue. Any suggestions for when I go as to what to say?
They should be able to tell you during a pelvic exam if the uterus is retroverted. If you feel like you have to insert your fingers in your vagina to push your rectum back to have a bowel movement, you may have a rectocele. It may, or may not have anything to do with a retroverted uterus. If you don’t have a certified ATMAT practitioner in your area, you may want to look for an osteopath who does visceral manipulation. I would also look into Restorative Exercise™ for pelvic alignment to reduce habits that may be causing extra internal pressure.
I really appreciate your post. I found out at the gyno recently that I have a retroverted uterus. He said it wasn’t an issue, but I just felt like that wasn’t true. I have had menstrual issues since this whole blessed thing started 14 years ago and I have a lot of the symptoms that you mentioned. I have been researching Maya Abdominal Therapy this afternoon, which led me to your site. I saw that you mentioned to someone that you can teach them via Skype how to correct a retroverted uterus. I’m wondering if that is still something you would be willing to do? I live in northern Utah and have not found anyone remotely near me that does this specific kind of fertility massage.
I no longer teach the Arvigo self-care via Skype. I do teach Restorative Exercise™ pelvic alignment via SKYPE which is essential for uterine positioning as well as the Chi Nei Tsang self-care. I’m teaching an Arvigo Techniques of Maya Abdominal Therapy self-care class in Boise next month. If you take the class, you will learn the self-care massage and much more. Here is the link to upcoming classes: https://alignmentmonkey.nurturance.net/2013/arvigo-techniques-of-maya-abdominal-therapy-training
If you can get at least 9 women committed to taking this three day workshop, I’d be happy to teach in your area. Contact me if you are interested 503-341-0663.
HI there, just found your article – thank you! I have constant constipation and bloating thanks to my retroverted uterus… Not sure if there is anything I can do to fix this? I’m over it. I noticed you no longer teach the massage via Skype. I am in Sydney Australia, is there anyone here you recommend? Kind thanks 🙂
I do see a few in Australia, but only only who is certified in Sydney. They don’t learn the retro techniques until certification.https://arvigotherapy.com/practitioners?lname=&city=&country%5B%5D=Australia
I don’t teach the Arvigo work via Skype, but do teach the Chi Nei Tsang and Restorative Exercise™ via SKYPE. In my opinion the Restorative Exercise™ is a crucial part for correcting retroversions and preventing them from happening again.
Hi Barbara, I am so happy I found this page. I am 8 weeks pregnant and went in thinking I had a prolapsed uterus and my OB did an ultrasound and found out that I have a retroflexed uterus pressing on my rectum making it very difficult to have a bowel movement. He said that it should go into an upright position as the baby gets bigger and that if it doesn’t he would have to sedate me and manually go up and move it into position which I do not want. Do you think your technique could help me?
Hi Jennifer, It’s been my experience that the uterus corrects itself usually by the fifth month when it gets heavier. Unfortunately, the retroverted techniques can’t be preformed during pregnancy. The basic Arvigo uterine massage can usually be applied by 20 weeks. Pelvic alignment and how you use your body is EXTREMELY important for encouraging correct uterine position naturally. If you need help with this, I offer Restorative Exercise™/pelvic alignment sessions via SKYPE if you’re not in the Portland area.
Thank you for the informative article. Please email me with the info of someone who does this type of body work in the Atlanta Ga. area?
You’re welcome. Thanks for reading. You can search the Arvigo website by location at http://www.arvigotherapy.com
I love your information. I get them off of facebook usually. Would it be ok with you if I shared the links of many of your posts on my website?
I also do ATMAT in Kansas
Joan
Hi Joan! Good to hear from you. I hope all is well with you. Absolutely, you may share the links. Thanks so much for passing along the information!
Hi Barbara, yes I am interested in the Skype sessions for restorative therapy. Can you email the details?
Thanks,
Jen
Details for those who are interested in SKYPE sessions. https://alignmentmonkey.nurturance.net/2011/now-offering-skype-appointments
Hi, the last time I had my pap smear the gynae mentioned that my uterus is closer to my back, but she said it’s ‘normal’. I went home and thought about that and remember some that I suspect could be the symptoms. During intercourse I could feel like want to have bowel movement, like something was pushing my rectum. I don’t have the problem when I have intercourse when I had BM-ed for the day. I have hemorrhoids since 2005, but it is until 2012 that I started to have hemorrhoids always flaring up during my menstrual. It was so bad that I even had hemorrhoidectomy to remove them. But even without the hemorrhoids now, I still feel burning sensation in my rectum whenever I have my mentrual, like new hemorrhoids are coming up soon. But I swear I had watched my diet after the hemorrhoidectomy, eating almost all vegetarian and avoiding meat, refined carbs and even not have a single constipation since then. Still I feel like me rectum is swelling during my menstrual.
Retroversions can put pressure on the rectum and interfere with hemodynamics causing pelvic venous congestion. There may also be a possibility of endometrial tissue in the space between the uterus and rectum. There’s a theory that retroversions can contribute to endometriosis.
YES! Utah often seems to get skipped over when I look for classes. I’m in Utah, too, and I’d love to learn more about Arvigo Techniques.
Hello,
I am following your thread about ‘Cervix being bumped during intercourse’, this happens with me in certain positions. I don’t generally have much pain during menstruation but I can become constipated for some days before my period. I have recently been researching more info after having seen a Maya Abdominal Massage practitioner. Though we didn’t speak about the position of my uterus. Your website is fantastic and make a lot of sense to me. Any feed back would be gratefully received.
Excellent post! Thank you so much!! I didn’t know there was hope for change! In my area there isn’t a Certified Arvigo practitioner. I do have quite a few VM3 folks here, though. Some are massage therapists and some are physical therapists. And some are part of the Wurn Technique group, which happens to be based here. Are certain of those preferable to others for trying to get my tipped uterus moved? I’ve been doing RE work for a year now, although not always consistently. I’ve worked with Lisa G. some. My uterus has been tipped for over 25 years, so I don’t know if that matters. Oh, and I had an internal ultrasound last year and the OB was shocked at how tipped my uterus was. :o/
Does a retroverted uterus is not easily to conceive or to get pregnant easily? My ultrasound shows that I had retroverted uterus. I want to correct it because I wAnt to have a baby. I want to have my own child.
Yes, retroversion can make it more difficult to conceive and may cause constipation and backache during pregnancy. It’s best to try to correct the position before trying to conceive.
I don’t know enough about Wurn technique. If you go to a VM practitioner who has completed VM3, it doesn’t matter if they are LMTs or PTs. I would call a few in your area and ask about their experience working with retroversions and see what other specialties they have to see what is a good fit for you.
Okay. Thank you very much! 🙂
I just found out about you only recently & you seem to be very dedicated to what you do.
I was told I had a retroinverted uterus years ago…2 children later & a prolapsed uterus in it’s last stage, I was wondering what you’d recommend. Not keen on getting the surgery, but this is getting to be an annoying problem, so I’m considering a pessary.
Would appreciate your feedback on this
Best Regards
Hi
I have a retroverted uterus that is blocking the passage if feaces and giving me extreme constipation
I now have a recticoele above causing chronic constipation
How can I telling to it’s proper position?
Can an osteopath help?
Clare
If you can see a practitioner who has completed Visceral Manipulation 3, I would do that. Not all osteopaths are trained in visceral manual therapies, so if you go to see an osteopath call first to ask if the can help you with your situation. Pelvic alignment is also important, so seeing a Restorative Exercise Specialist™ or a Physical Therapist who specializes in pelvic alignment and the pelvic floor would also be important.
Dear Barbara
I am 66 yrs. old. Recently I went to my GP for a physical and pelvic exam. The last 2 times I had this done (different doctor) it was extremely painful but completed. This time the doctor said my uterus is too far up.
This could explain why I have severe lower back pain and a feeling that things are crowded. For example: I cannot have a BM unless my huge bladder is emptied. Right
Hi,
Thank you for this article. It feels like home.
4 years ago,my gyno. confirmed to me that there was no problem with my uterus leaning on the left, on top of my ovaries. He was crazy! I was in extreme pain every month right before and during menstruation.
It got worse!
I am late 13 days,very bloated and cramping!
Any idea what to do to massage the uterus back in place?
Thank you 🙂
Now, I am late in my menstruation for 12 days
Unfortunately, it’s best to learn one-to-one on how to correct uterine position using massage. There are too many factors to explain clearly in an article. Check the arvigotherapy.com website for a practitioner near you, or barralinstitute.com for someone who has completed Visceral Manipulation™ 3 (pelvic organs). If there isn’t anyone near you, I offer SKYPE appointments. I can’t teach the Arvigo self-care via Skype, but I can teach you other methods of uterine alignment/abdominal massage. https://alignmentmonkey.nurturance.net/2011/now-offering-skype-appointments
Hi Barbara,
I have retroverted uterus and was told by my gynecologist that my chronic constipation and back pain could be related to that and possible endometriosis. I’ve had 2 kids in 2011 and 2013 but uterus still quite tilted, with symptoms worse than pre pregnancy. I now live in China and am interested in a Skype class. Please let me know how to proceed.
Best,
Millie Shih
Hi! I just want to ask if retroverted and retroflexed uterus can be pregnant? Because have that case and i’m married for a year and i’m not pregnant yet. I’m already depressed! please help me what to do! thanks!
please, my case is this, I have shift in my womb since the birth of my second son in 2015. pains during ovulation and sex several efforts to normalise it did not work. I went for massage for local massager for about six months but only reduce the pain but not completely. I touches it any time I deficate soft and round. I am just 40 years old, it is a burden to me, please what can I do?
Hi Barbara, Where are you located? And should any good ayurvedic clinic be able to undergo that massage technique to return the uterus to its correct position?
I’m in Portland, Oregon. The techniques I know for correcting retroversions are not Ayurvedic, they are from the Maya tradition and Visceral Manipultaion™. I may use an Ayurvedic hip massage to relax the pelvic area, but not specifically for correcting the uterine position.
I have a tilted uterus u was told can it cause pressure and cramping for a week…also certain positions are very un comfortable if I see a LmT that specializes in This. Could it change its position…I’ve never had these types if cramps and pressure before also I was told by a chiropractic my pelvis is tilted too help
Hi Barbara,
First, thank you so much for the incredible information on your site; invaluable and so generous and kind of you to share it freely! I’ve had severe cramps for years, with vomiting, cold sweats and so on, which I’d learned to manage by overdosing (as recommended by doctors) on ibuprofen every month. I have been told on various occasion that I have a ‘backwards’ or ‘tipped’ uterus, but of course that it’s normal / common and not an issue. I’ve also taken multiple courses of antibiotic cream injected to treat a foul smell (that was also confirmed to coincide with very high bacteria), but after multiple courses which didn’t change anything my obgyn concluded that it must be ‘normal for me’ (even though she said it was not normal when prescribing the cream). So, my first curiosity is if you think there may be a connection between the bacteria (from the rectum?) and my ‘tipped’ uterus? Another question, do I need to know what the specific uterus position is in order to seek treatment for this? Related to that, will I know if it has been corrected by treatment or how would I know? There are ATMAT providers in my area, but the results mentioned are less specific than yours, in which you say that you can correct this issue often in just one treatment (I wish I were in Portland!)! Lastly, you mention that one should give at least three months before trying to conceive after seeking treatment. I have been doing acupuncture for half a year for infertility, so would like to avoid waiting and am just wondering if you could share more about the reason for the need to wait to try to conceive after? Thank you again for the information!!
Hi Kim,
To answer your questions: 1.From what I was taught by Dr Arvigo is that toxins from the rectum can seep into the vagina when the uterus is stuck in a retroverted position. Lymph and blood flow can also be impeded creating an environment for infection. 2. No, you don’t need to know your specific uterine position in order to seek treatment, sometimes it’s helpful, but not necessary. You don’t even need to have a malpositioned uterus to benefit from the treatments. 3. You will know if there is a correction when your symptoms change, or you OBGYN tells you it has changed. 4.Sometimes retroversions can be corrected in one treatment, but those cases are when it hasn’t been going on for very long. It usually takes at most 4 sessions over three months of receiving treatments and doing the self-care massage. If you see a certified practitioner you should be fine. ATMAT providers don’t learn the retroversion techniques until they take certification training. Keep in mind some retroversions can not be corrected with manual therapy due to severe scar tissue or adhesions.In these cases, I believe the symptoms can still be improved using manual therapy. 5. You will find you answer here…https://alignmentmonkey.nurturance.net/2011/preparing-to-get-pregnant/
do you still give class to possibly help correct a retro flex uterus?? I would love to learn.
i am tired of have pain. It’s been about a year since I started to notice a change. I got diagnosed about 8 months ago.
I have been having pelvic pain and pressure typically in my left side near my hip of I’ve had this pain twice in the last 7 months now, the pain shows up and stays for a few months and then goes away. I also had a miscarriage 6 months ago, that’s when my first left ovarian cyst was discovered. The pain went away after a few months and returned last month, my doctor sent me for an ultrasound where they have noticed a cyst again on my left ovary. The cyst is noted that it is 1.8 cm with a minimally complex single internal septation that demonstrates flow. On the same ultrasound results it states I also have a retroverted, retroflexed uterus. It also states I have mildly prominent adnexal veins bilaterally which are greater on the right, noted here it could be a nonspecific finding, however seen with pelvic congestion. I am 27 and a mother of three wanting to have a fourth, my obgyn has ignored anything other than the 1.8 cm cyst. I still have my pelvic pain 6 weeks and 1 day later the pain unfortunately this time the pain has caused more problems. My symptoms are sudden cramping when the start of my period, pain when using the bathroom, pelvic pain/pressure in left hip region, pain during sex, cramping without period, and headaches. I currently take 800 mg of ibuprofen which do nothing for my symptoms. This is the only article I can find on this issue that addresses all of them. I was wondering if many doctors share your same thoughts and findings and what steps I should take to get this issue resolved. After reading this article it has scared me and has made me decide to put my plans of pregnancy on hold till I can address this issue. Thank you so much for this very informative article, it was really the only informative one I have found.
Great article! I was very interested.. I may have a titled uterus I have all these symptoms. My problem is I maybe pregnant and almost due. I can’t get confirmation because of negative test, and blood testes. I even grew a big bump on my right side.. I tried getting a referral to obgyn, still not working for me. This sucks for me on this end..
I am a desperate, post-menopausal 51 year old looking for an answer to sciatica/si joint/right buttock/pelvic pain. I have been to ortho doctor, who did MRI that revealed nothing substantial related to a disc or spinal problem. Have been seeing chiropractor for 3 months now but still have problem. I cannot sit without pain. I have been on a mission for nearly a year to find my problem. Never had a moment of back problem ever. Was told for the first time ever last August by my ob-gyn that I had a tilted uterus, and I am would love to know if this or some other female organ issue could be my problem. Something in my heart says it could be. Will appreciate any advice/comments.
Hi Tracy, Have you read my article about sciatica? I talk about causes other than disc issues in the article: https://alignmentmonkey.nurturance.net/2016/sciatica-your-disc-may-not-be-the-cause/
For the tilted uterus, could one of the symptoms be missing your period often?
hii i am marisa and i have been told that i have retroverted uterus. i am 34 years of age and have being trying to get pregnant ,so i was also told that i have poly-cystic ovaries.
does surgery hurt or does it have any consequences?tilted uterus what happens if I’m not treating it?I’m sooooo scared
Hi,I was told i have a tilted uterus i have been ttc #2 for 10 years sex “doggy:” style makes it very uncomfortable and makes me feel i have to pee all the time. i also was told i have a slight overactive bladder i am now getting constant cramping like period cramps .my pelvis is tilted as well. are there exercises to help this? i just got casted for orthotics , i am top heavy too 38 ddd 🙁 i just want to feel normal again, was scanned for cysts no cysts, ob/gyn thought i had ic,uro said does not see any or think i have that bc i pee all the time i do drink a lot of water and am on a strict diet i was thinking of getting a massage to correct this,how does this work?thank you so much!
This is the most amazing thing I’ve read thank you. I knew my mother had a retroverted uterus but that didn’t mean much to me, and it’s been mentioned to me at every ultrasound I’ve had with my four pregnancies. I’ve miscarried alternate pregnancies and it’s all been viewed as fairly normal. I’m wondering if the tilted uterus might have created a sub-optimal blood flow or if it’s affected my progesterone levels.
I’m reading with interest your comment about the retrograde blood in the abdominal cavity. My last miscarriage was bizarre with the length of time it took to stop bleeding and a scan showed fluid in my abdomin, but as it wasn’t ectopic no one was concerned.
Man I feel really frustrated that no one talks to you about how your physiology affects your health :/
I want to get pregnant but i also have retroverted uterus and surgery is too expensive. I dont know what to do now because I saw an article stating that its hard for me to get pregnant. 9 months of trying to get pregnant, im losing my hope. 🙁 Is there other easy way? What about exercise? Manual positioning? Pls help.
Yes, I’ve outlined my approach to correcting retroverted uteri using exercise and manual therapy in the article
how much the procedure cost me?
My rates are listed here. http://nurturance.net/rates/
I’m glad I found your website. I have a retroverted uterus with several small fibroids. I have been having sever sciatic pain right after my period and also rectal pressure that usually last a week and then goes away. I have had CT scans, ultra sounds and x-rays of my back and the doctors say that cannot find a reason for my back pain…I asked if the retroverted uterus could be the problem but they said no as the pain comes after my period. They think it is something gynecological but don’t know what… I’m at my wits end as the pain seems to come all the time now. I would like to know if you ever heard of the pain coming after a period. I have had to children and it seems after my second child all my problems stared which was 5 years ago. I would like to try some exercise to see if they help…PS I also have heavy periods…
Hi Linda, Have you read my sciatic article? Here is a link. https://alignmentmonkey.nurturance.net/2016/sciatica-your-disc-may-not-be-the-cause/
You may want to see a Visceral Manipulation™ therapist who has completed VM3 to rule out surrounding structures being the cause. An Osteopath who does manual therapy may also be able to help.
Another possibility is a corpus luteum cyst, which is a type of ovarian cyst which may rupture about the time of menstruation.
a third possibility is uterine/rectal adhesions. Which don’t always show up on ultrasounds. Either way, I recommend manual therapy (unless you have an IUD).
I have a retroverted uterus, just found out when I went for my first abdominal ultrasound at 10.5 weeks (it did not come up at my transvaginal ultrasound at 6.5 weeks – nor has it ever come up at a gynecologist). I have heard that sometimes pregnancy causes a retroverted uterus and then itself corrects. But I am interested in doing exercises to help make sure it aligns itself correctly to deal with back pain, make sure blood is flowing well down there, and reduce any risk of miscarriage. Are the exercises you recommend specifically known to be completely safe for pregnant women? I did a bunch of prenatal pilates exercises from a youtube video one day and then had a abdominal cramping for 24 hours afterward. I can’t help but wonder if my uterus was in a fine position (since I was never diagnosed as having this before) and then somehow I shifted it backwards. I wish I had a better sense of how abdominal muscles actually interact with the uterus. I keep hearing this general tip of “strengthening your pelvic floor” but I have not heard any explanation of how the abdominal muscles directly relate to and move the uterus one way or the other. If you have any insight on this specifically it would appreciated and I would be possibly interested in a skype consultation. How much do you charge?
You may have shifted your posture since pregnancy which may have influence uterine positioning. The main thing I would watch out for is posteriorly tilting the pelvis (tucking under). A posterior tilted pelvis may encourage a retroversion. The other possibility is that it was retroverted to some degree before, but not enough for the doctor to mention it and then when the uterus got heavier it increased the retroversion or became more apparent. Many times they don’t mention retroversions because they don’t think it’s a big deal and they see it so often.
As far as the Healthy Pelvis exercises in Katy Bowman’s program, the answer is in general, they are safe for pregnancy, but it depends on the current state of the individual. My recommendation would be to work one to one with a Restorative Exercise Specialist. If you aren’t in Portland to see me in person I charge $95 per hour for Skype sessions.
This information was EXTREMELY helpful, as I will bring it up in my next visit with my PCP. For years I have been suffering from 4 out of the 9 symptoms of Retroverted Uterus. Those symptoms are also accompanied by anal spasms at times. Which seem to just happen spontaneously. Every day I am in pain. The only relief I seem to get it soaking in a hot tub. But even that is seeming not to be of much help as I am only able to utilize it when I am home. When I am at work I have to suffer and bare through the pain. I’ve had 2 colonoscopies and 1 laparoscopic surgery. These doctors don’t seem to really want to find what’s wrong with me, as they continue to shift me around and pass the responsibility of care. I had to do my own research to find this article and I’m glad that I did. Can you please please please give me any feedback?
Hi Dana,
I’m sorry, but I don’t have enough information to give you feedback and it wouldn’t be appropriate in a blog forum. All I can say is that symptoms similar to retroversion can be from other causes as well. First I would find out if you actually have a retroversion, what degree of retroversion and whether it’s adhered to posterior structures. Another thing to rule out is pelvic floor issues, like a hypertonic pelvic floor. Seeking evaluation from a pelvic floor PT or someone trained in Holistic Pelvic Care should be able to help you with that. And if you do have a retroversion, a certified ATMAT practitioner of Visceral Manipulation™ therapist trained in VM3 should be able to help. Some Osteopaths also do manual therapy.If you need assistance with Restorative Exercise for pelvic floor health I can help you via Skype. Best of luck to you.
Hello barbara,
i am trying to conceive from 1 year and i found that my uteres is on back side after my visit to gynacologist for TVS test. she said there is no problem in conceiving if uterous is backward. please help me on this. i have reached your link to find practitioner in my area but there is no one. please help me on this.
It is possible that the degree of retroversion you have may not interfere with your ability to conceive. But there are ways you can work to improve uterine position if this is a concern for you. I do offer SKYPE sessions. I don’t teach the Arvigo® work via SKYPE, but there are other things I can coach you on that may help. https://alignmentmonkey.nurturance.net/work-with-me-2/
Hi thank you so much for this I recently received 4 abdominal massages age today she said my uterus has been moved back I am just paranoid it will slip back again she asked me to go back next month as she wants to know how my next menstration goes ? Can it slip out again ?
Thank you so much for your advice and help
Sorry to read about your Mum
Hello Barbara,
I had an ultrasound to check out how everything was “down there”, because I have hormonal issues. Everything was fine, except I was told my uterus was slightly tipped, which I was told isn’t a big deal. They didn’t tell me which way it was tipped though, and I did not think to ask. Now that I am researching about it, I wish I had. Would that explain why during my period I bleed to the right side of the pad all the time and not evenly? Also would I be able to use a Diva cup with a tilted uterus?
Hi Melissa, The cervix can tip independently of the uterus. For instance, if the right cardinal ligament is restricted, it could pull the cervix to the right while the uterus could be tipped in another direction.That may explain the right side bleed on the pad. Have you looked at your cervix? My other thought regarding bleeding on one side of the pad is that perhaps it’s gait related?
Yes, it’s possible to use the Diva Cup with a tilted uterus, if it’s comfortable. It might not be depending on the degree of tilt.
I have never looked at my cervix. I don’t even know how I would go about doing that.
Some women use a home speculum and mirror, but a speculum isn’t always needed to see the cervix.
Hi! I was so touched by your article in many ways. I have a retroverted uterus and my mother had a prolapsed uterus, which first started as a retroverted uterus and after a really bad fall and as a result of that she had the prolapsing problem. Iittle before she died, i became aware of all the health problems that it was causing her such as bad circulation, varicose veins in her ovaries… and as you i wish i had been able to help her.
Hello, Barbara! Do you have any information hove does MIRENA (birth control ‘device’) influence uterus or woman’s body?
I’m not a fan of hormonal birth control. Dr. Lara Briden wrote a balanced article on the Mirena IUD here,http://www.larabriden.com/pros-cons-mirena-iud-natural-health/.
I also don’t recommend IUDs with retroverted uteri. I’ve seen too many women experience extremely painful periods and backache until they had the IUD removed.
The IUD is an irritant to the uterus. Uterine manipulation can’t be done with an IUD present.
Hi, Barbara, your website is fascinating and has caused me to question my gynaecological health! Random background info: When I was pregnant with my second child I was told my uterus tipped back – I’ve always had constipation prior to my period and my only pain during my period these days is a dull ache in my lower back.
I’m a long distance runner and did a 20k run on Sunday, which naturally resulted in a few aching muscles, my right hip particularly. I followed the run with a yoga class on Monday evening to help loosen me up. Later that night, my hip was still achey so I gave myself a really good massage, tackling a number of tight spots in my sacrum, lower back and around the hip. My period arrived today (Tuesday) and is super heavy – I’m talking lots of big clots and a new super tampon needed every hour or two. After reading your website, I’m now wondering if there’s a connection between the tipped uterus, the massage and the heavy period. Your thoughts would be appreciated.
If the uterus has lost tone or can’t function properly due to a malpositioned or flexed uterus.
I’m assuming you are referring to the Arvigo® massage. The massage shouldn’t cause heavy flow. Kepp in mind that you shouldn’t do abdominal massage while menstruating.
Did you sauna or take aspirin after your run? That can also cause a heavier flow. As well as blood sugar imbalance. I wrote about other causes here: https://alignmentmonkey.nurturance.net/2014/heavy-menstrual-bleeding/
Hi barbara…thank you for the article. I’m 31 yrs old and i want to get pregnant…but i have pcos and retroverted uterus…i have menstrual problems…sometimes its heavy sometimes, sometimes less than normal…my ob gave me provera to clean my uterus but it lead me to having 2 mentrual cycles in a month…what shoul i do? My ob is out of the country right now…this happened two times already…please guide me…
I’m so sorry Jennifer, the human body is too complex to give specific advice. I recommend following up with another physician since yours is out of town. They usually have someone covering their practice while away.
As for the heavy bleeding, I wrote an article on that, search “Heavy Bleeding”.
For PCOS check out the book Woman Code by Alisa Vitti.
For the retroverted uterus seek out help from a certified Arvigo practitioner.
Hi Barbara…Most of what I’m reading online talks about retroverted uteruses causing lower back pain during periods or pregnancy. Could it be the cause of my chronic back pain? My lower back hurts most of the time, but is tons worse during menstruation. Another question — it’s always worse in the morning, and gets better as the day progresses. Is there something about lying down all night that could trigger the pain and make it worse? Thank you for your article. Nice to get some good info!
I suspect you have something else going on. Usually, a retroversion will cause pain right before and during your period when the uterus is heavier. Although a uterus that is fixed forward can pull on the uterosacral ligaments and cause low back pain. Prolapse can also cause low back pain. Either way, it may help to get an Arvigo® treatment. Abdominal massage can help relieve back pain and 50% of the Arvigo® treatment is also on the back, hips, and sacrum.
Thanks so much for this article. I was wondering what your opinion is on hypoppresive exercises helping to shift a retroverted uterus foward. I have a retroverted uterus and cervix. I have seen an arvigo specialist and a visceral manipulation specialist and I was wondering if its possible to correct a tilted cervix? and how?
I honestly can’t see how hypopressives could shift a retroverted uterus. My thoughts on Hypopressives is right along with what Julie Wiebe wrote about in this article, http://www.juliewiebept.com/individual/hypopressives-ive-got-questions/
Sometimes the cervix will correct when the uterus does, or independent of the uterus (different ligaments). Did your Arvigo® practitioner do the retroverted techniques with you?
Not knowing you it’s difficult to say what would be best, but I always look at pelvic alignment in relation to the rest of the body, work around the pudendal nerve (Hortense’s point), and sometimes refer out for Holistic Pelvic Care (intervaginal work).
She taught me a self massage at home. She would have me lay on my side and try to scoop my uterus forward. Also did a hip massage with a salong to shuffle it forward and with a cupped hand hitting the sacrum. What intervaginal work can be done? And how can I find a practitioner to help with this?
Typically we recommend treatments and self-care for 3 months. If thick adhesions are holding your uterus in retroversion, the techniques probably won’t correct the position but should help with blood and lymph flow in and around the uterus and many associated symptoms. This is the website of the creator of Holistic Pelvic Care, http://www.wildfeminine.com/. It doesn’t look like she has a list of practitioners, but you could google “Holistic Pelvic Care”.
Thank you. I have found an holistic pelvic care practitioner. Could a rectocele repair cause these adhesions? About 5months after surgery is when it moved after I lifted something that was too heavy for me and I didnt get symptoms till around 10 months after.
Yes, surgery usually does cause adhesions. The first phase of scar formation starts with the inflammatory process in the first 48-72 hours of the trauma. The proliferation phase lasts up to 6 weeks and the remodeling phase, or maturing phase may last up until two years.
I have a question how can I contact you by phone. Where do you provide your private practice?
This article was very helpful ! I am 29w1d pregnant with triplets and have a retroverted uterus. I was never diagnosed with anything. I got 1 positive pregnancy/ultrasound test at 5w and every since all my tests and ultrasounds have been negative. I still feel kicks, movements, I’ve gain 60lbs, my stomach is huge and all the doctors keep saying I miscarried because my tests are coming back negative. The givd me a test then kick me out. I’ve bled every 28days since my last normal cycle 8/1/17. Didnt bleed in January or February and my tests are still negative but still growth and stronger movements and kicks DAILY. The pain is horrible at times esp when I would spot….Any advice for me? Any recommendations? Would You Like To See For Yourself? I have pictures, videos, medical records. Honestly I’m scared to death, I’m constantly crying because I dont know what else to do. Please Help Me Im Crying Out Loud Please !!
Dear Shantelle,
I wish I could help you, but your situation is out of my scope of practice. I recommend that you go back to your doctor for guidance ASAP. Press them for answers, don’t leave until they have a plan or referral for you.
Barbara, thank you for being a caring and wonderful resource.
I am 57. Never pregnant. I have known about my “tilted” uterus for a long time. I am in great shape and very aware of bodily changes. I have had two incidences of diverticulitis in less than two years and am wondering if my uterus is in a position where it’s causing issues with my colon. I just had a colonoscopy. I have very mild diverticulosis. Also after the last diverticulitis I have been aware of increased pressure on my pelvic floor. If I do Kegels the pressure goes away but I am always aware of some pressure “down there”. Actually when I ride the bike at the health club it is decreased greatly. As well as when I do certain stretches. Sorry this is so lengthy. Any thoughts you have would be appreciated. Thank you.
I can’t say specifically what is happening with you. The body is too complex to say without a thorough intake and evaluation. In general, a retroverted uterus has more of a risk of becoming prolapsed because of its angle and overtime the ligaments become weak if not loaded correctly. I would get evaluated for uterine and/or rectal prolapse and see an ND for getting to the root of the diverticulosis. It’s possible the uterus is irritating the rectum, but I’m not sure if it could be the underlying cause. Either way, the pelvic positioning exercises in the Healthy Pelvis class are generally helpful. I’m guessing the biking is helping to alleviate symptoms because it may be positioning your pelvis out of a posterior tilt.
Dear Barbara,
Thank you very much for your marvelous article! I have a retroverted uterus (was born with it, as far as I know…), and I have all of the symptoms that you have described here and tons of pain. Some months I can barely take it and feel like I have the flu– totally saving my white flag. I’m very glad to hear that it is not just me, that there is a logical reason behind my crazy symptoms, that I am not crazy or weird, but also sad to hear that others suffer with the same problem.
I would love to find a way to get it arighted to cure all of these symptoms, although I don’t think you live in my area. Would you happen to know of any practitioners who are certified in what you are and in the principles described in your article in the NYC area? I would be most grateful.
Sincerely,
Kristine
Hi Krisrine, You’re welcome! Have you looked on the Arvigo® website? You can search for a practitioner in your area. Make sure you look for someone certified.https://www.arvigotherapy.com/
Best of luck to you. I hope you get some relief soon!
Hi I live in Jaipur city of India. I have gone through your article and all the comments. I suffer from retroverted uterus. I think it’s the consequence of an abortion I had two years back. We dint want a fourth child. I have all the symptoms and I am in a lot of discomfort and pain. I got an MRI done and found about the retroverted uterus. I have consulted the senior most gynecologists of my city. All of them tell me that it’s not a big problem. I guess only the sufferer knows the magnitude. This problem is affecting my life adversely and I desperately need help. Please help me. Is there an Arvigo therapist maya abdominal therapy, anywhere in India.
I forgot to.mention PID, continuous discharge pain, recurrent UTIS, vaginal infection. I have taken antibiotics prescribed by doctors for about two years now, I took homeopathic and ayurvedic medicines but to no avail. Please help.
Thank you SO much for this article, I have suffered from extremely painful periods for many years and have tried everything under the sun. I recently went to the ER and had an ultrasound done and she mentioned my tilted uterus, she never mentioned it could be what is causing all my pain though! Glad I found you, wish I could come visit you, but I did find a certified practitioner closer to me in Hawaii. Excited and hopeful to try this out!
Shriya, I’m so sorry to hear about your suffering. It sounds like the root of your pain is probably more than the retroverted uterus. With PID there are likely adhesions present. The adhesions may even be responsible for the retroversion. There aren’t Arvigo® practitioners in India. I would suggest finding a practitioner who specializes in a gentle form of abdominal therapy to address the adhesions. Although, of course, it’s impossible for me to say what is best for you, not being able to see you in person. You may also want to try castor oil packs, and ginger compresses. Focus on an anti-inflammatory diet. These supportive techniques may not solve the problem but should help with the pain and reduce chances of more adhesions from forming.
I’m glad you found someone near you! Make sure they teach you the self-care massage. It’s a very important piece of the healing process. Try to stay consistent with it for at least three-months as directed by your practitioner.
I just found out today that I have a tilted uterus. very active, which was probably the reason I carried till the end, but now that I have been out of routine I have had three miscarriages back to back. I have all they symptoms listed. Low back pain (sciatica), endometriosis, fertility problems, intercourse and ovulation pain, and constipation.. I have always had a retroverted uterus. would it still be possible to correct this?
Hi does a retroverted uterus affect the severity of menopausal symptoms.
Thanks Carolyn
So I am 15 and I have a tilted uterus and have gone and seen a special doctor about it that uses the massage technique. I haven’t yet gotten my period would that play a role in that?
Thanks
A tilted uterus may be perfectly normal at your age, but it depends on if you are having symptoms related to uterine position, your uterus is immobile, or if the malposition is due to a trauma. There are normally varying degrees of positions in prepubescent girls. The uterus changes position in response to puberty. Another possible cause may be the fact that prepubescent girls are still growing which may have an influence on positioning.
Since your doctor is treating you for a tipped uterus, I’m assuming there is a good reason. In theory, a malpositioned uterus may influence hormones in some cases. But there are other reasons (diet, underweight) you may not have gone through menarche. It could also be totally normal that you haven’t started a period yet, some girls start later than others. I had my first period at age 16.
Your doctor would be best at answering these questions since she has your thorough history.
Hi, I’m a 24 year old with extremely retroflexed uterus. On my menses days, there is extremely heavy feeling between the vagina and rectum. I can feel what feels like veins bulging. My cervix is also very low lying. And when I have a bowl movement getting ready to happen i get excruciating pain. None of the doctors I’ve been to were concerned. Any idea on relief? My uterus retroflexed after I gave birth to my daughter, naturally. I don’t have access to a practitioner for these massages.
If you don’t have an Arvigo® practitioner near you, what about a Visceral Manipulation™ practitioner (VM3) or osteopath who does manual therapy?
Pelvic position is extremely important as well, have you done the Healthy Pelvis course?
Can you help with retroverted uterus?
Am really encouraged by your article and it gives me hope. I was diagnose with a retroverted uterus when i did a scan three years ago. I felt it was normal as i have no symptoms or discomfort whatsoever. I got married two years ago and still unable to conceive. that makes me to research about every thing that could cause it.
Am desperate for a solution to reposition my uterus and hope to conceive and give birth to my healthy children.
i need your help with the self massage as there is no practitioner in my area.
Hi there Barb,
I was diagnosed with retroverted uterus last year. Me and my husband got married and trying to conceive and noticed that I was having a hard time getting pregnant. My fertility specialist advised that having a retroverted uterus was normal and that many woman who have retroverted uterus are able to have children. My fertility specialist went on to giving me fertility drugs like letrozole, I continue to get blood work done and ultrasound and still not getting pregnant. It’s been 6 months now and no pregnancy. I keep telling them, well maybe it’s because of the position of my uterus, and the fertility specialist told my to stay off google. I’m really frustrated.
Thank you for sharing this information
Hi
I heard my doctor telling a colleague that I have retroverted uterus while performing a transvaginal ultrasound,I have been trying to get pregnant for 3 years after my first baby that was born after 4 years of trying,can my retroverted uterus cause my infertility?
Hello,
Is it possible to have chronic constipation due to retroverted uterus ?
My guess is that if the retroverted uterus will push against the rectum and “block” the normal flow of the rectum ?
Is that possible ?
It’s known that during a rectal examination, the doctor can feel the uterus with his finger…