I used to pee my pants (just a little) when I “walked like a lady” (legs close together). No, I’ve never given birth, so I can’t blame it on that. Many women experience incontinence who have never given birth. Incontinence is not a natural result of having a normal vaginal delivery (that would be a pretty crappy design of the human body). Incontinence may be a sign that you have a weak pelvic floor because you’re not using your body the way nature intended. Excessive sitting, positive heeled shoes, cultural messages (walk, sit, stand like a lady) have all shaped our minds and bodies. We are how we move…or don’t move.

The following information is really about me playing a pee detective.


Drop a plumb line from your ASIS, it should fall mid-point through the knee and ankle.
When I started walking with my feet the correct distance apart I no longer had a problem with incontinence (or the feeling of urgency). Walking with my feet pelvis width apart also encouraged my femurs out of internal rotation. Notice how my knee is a smidgeon the inside of the plumb line, not because I need to widen my stance, but because my femur is internally rotated.
Walking with my femurs in neutral helped to support my pelvic floor (the pelvic floor does NOT work in isolation). The result I experienced wasn’t just that I was able to “hold it in” better, but the actual urge to pee went away. It felt as if something lifted off my bladder. Perhaps the change in femur position also lifted my uterus off my bladder? BTW, I’m not positive femur position can affect uterine position, I’m just playing detective with my own body. This is how I came to the conclusion:
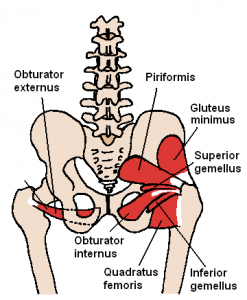
The cardinal ligament is known as the main supporting ligaments of the uterus, upper vagina, and cervix. It attaches in a circular pattern around the cervix and moves laterally to the obturator fascia along the pelvic sidewalls. Inferiorly it is continuous with the fascia on the upper surface of the levator muscles. The obturator internus attaches to the medial aspect of the greater trochanter (see image below), so this got me thinking that a neutral femur might help support the cardinal ligament. It also makes me wonder if “incompetent cervix” has to do with a disruption of flow through the ligament to the cervix due to poor alignment or tight pelvic floor. I haven’t come across any studies suggesting my femur/uterus hypothesis, I’m just going by how it feels to me. If you know of any studies related to the uterine position and femur position, let me know. In the meantime, all I can say is pelvic and femur alignment is working for me!
Please don’t force “alignment”. Walking should be reflex driven. I can’t emphasize how difficult it is to know where you are at when just starting out on the alignment path and how easy it is to force “alignment” to the detriment of your tissues. That’s why working with trained in whole-body alignment is so important. I recommend working with a Nutritious Movement™ certified restorative exercise specialist.
It’s important to build up your lateral hip strength while standing first and avoid pushing your body into doing something it’s not used to doing during gait. This is some of what I did to strengthen my lateral hip musculature. I’m including it here as a note to myself and as homework for the clients who I already work with. pelvic lists and monster walks and I worked on getting my femurs out of internal rotation. And of course, foot position and shoe choice is a great place to start.

Look at me now! No leakage. 🙂




Thanks Barbara.
I’ve done the plumb line from the side, and try to put my feet “hip width apart” when I line everything up, but it never even occurred to put these two together. D’oh!
Thank you for all the wonderful information you provide! i wish I had found your site before I got pregnant, but am really glad I have it as a resource now.
I have the “Down there” DVD now and do the exercises you post!
BTW what kind of shoes are you wearing. They are really lovely?
Thanks!
Thanks so much Jenny! I’m wearing Jambu barefoot shoes.
Like the post, like the shoes. Thanks!
Thanks for this info Barbara, I have just started looking at the first 2 hours of Katy’s webinar. As a pilates person, I already know about hip width apart legs but this gives me a way of measuring the optimum distance which
is why I first looked at Kay’s info anyway! YAY!
ie: to get a more biomechanical understanding of where we are supposed to be.
Thanks Alignment Monkey.
Hi,
I just found your site from Katy Bowman’s blog. I found her blog and have read her books starting this past November. I had no pain prior to this but was just really interested in preventing problems. I had been walking 3 miles a day and I have continued that. I stopped working out after reading her books/blog in favor of walking more and because I was worried that I had wrong alignment for lifting/HIIT intervals. I feel like I have adjusted quite a few things (not tucking my pelvis, sucking in, going barefoot more, not thrusting ribs) and I try to do some of her stretches and releases. However, in the past month and a half I have developed pain/tightness in my left hip/lower back and I cannot figure out what is causing it! It frustrates me to no end because I thought I was making improvements in my alignment and now I have this pain. Any ideas? Thanks!
I have no idea….perhaps you didn’t give your tissues time to adapt? I recommend getting a session with a Restorative Exercise Specialist so they can evaluate your alignment, how you are moving and doing the corrective exercises.
Okay, thanks for your response. Also, when I walk with my feet wider apart like in this post, it feels like I look like I am waddling or have a diaper on or something! Maybe I have them too far apart, but it just feels so weird.
I wouldn’t force walking with feet ASIS width apart. It shouldn’t feel like a waddle. I would have a RES evaluate your stance and give you correctives to work on. Walking should be reflex driven, not forced.