When most people think about sciatica they think of compression from the L4-L5/S1 or piriformis tension.
The lasegue test is a common test for sciatic nerve pain resulting from lumbar disc compression. To preform the lasegue test the patient lies supine (on their back) with legs straight and the practitioner passively (without help from the patient) lifts the leg. If lifting the leg between 30 and 70 degrees elicits pain in the leg it is considered a positive result for disc compression. However, if the practitioner inhibits (compression in a particular direction depending on their evaluation) the pelvic ovarian zone and it produces immediate improvement in hip flexion by up to 30 degrees it’s an indication the origin of the pain is not a disc problem but is rooted in an ovarian or uterine restriction, displacement (especially retroversion) or enlargement. Enlargement may be from a fibroid, adenomyosis, venous congestion or large cyst.
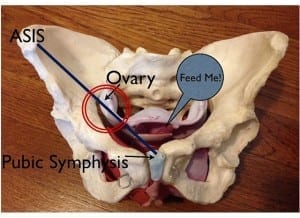
Pelvic ovarian zone highlighted in the red circle. The “feed me” has nothing to do with this information. Just me being silly.
Pelvic ovarian zone: If you draw a line from ASIS to pubic symphysis the ovarian zone would be in the lower third.
ovarian restrictions can also cause low back pain typically in the premenstrual phase. If movement increases pain then the root may be more mechanical in nature and involve disc problems. Ovarian restriction causes of low back pain wouldn’t cause more pain with movement.
Abstract:
“The principal author was confronted few years ago with the case of a 38-year-old woman with a 5-month history of ill-defined L5 sciatic pain that was referred to an orthopaedic department for investigation and eventual surgical treatment for what was suspected to be herniated disc-related sciatica. Removal of her enlarged uterus found unexpectedly close to the sacroiliac joint upon lumbar MRI abolished her symptoms. Review of the literature showed that the lumbosacral trunk is vulnerable to pressure from any abdominal mass originating from the uterus and the ovaries. Physiological processes in the female patient and gynaecological diseases may be the source of sciatica, often not readily searched for, leading to fruitless investigations and surgical treatments. The aim of the paper is to highlight gynaecological and obstetrical causes of sciatica and sciatica-like symptoms. To prevent unproductive expenses and morbidity, a thorough gynaecological examination should be done even though neurological examination may be suggestive of a herniated intervertebral disc, and the cyclic pattern of pain related to menses should be routinely asked for.” READ full article HERE.
“Some kinds of visceral pain go as far down as the lower leg. Pain of tuba-ovarian origin should never extend past the ankle. The cutaneous tibial ramus circulates particularly in the internal calf and irritation of this nerve can be confused with sciatica. The saphenous nerve (branch of the femoral nerve) has a posterior terminal branch in the leg which is related to the saphenous vein. Irritations of this branch also produces similar symptoms” (Barral, 1993).




Could you give a more details on how to perform the lasegue test while applying pressure to ovarian zone. What kind of pressure are we talking about? This is very interesting. I visited you when I was in Portland one time and I really wish you were closer.
Please say more about that test and how to distinguish gynecological issues. Two spinal injections did nothing, so now I’m looking at spinal surgery but the pain is cyclical. Spinal Drs think I’m nuts when I say that, and Gyn thinks I’m nuts when I say ovulation on right side causes back agony and severe sciatica. I also have small fibroid on back of (retroveryed) uterus under right ovary.
Hi Laura,
I recommend seeing a Visceral Manipulation™ practitioner, or an osteopath who does manual therapy (not many do in the U.S.), they should be able to isolate the cause of your pain and work with any restrictions. You could also seek help for your retroverted uterus from a certified Arvigo® practitioner.
Good news! I have suffered with sciatic nerve pain for 2 years. I thought I overdid it in my workouts. I have an inverted table to relieve pain (which does help if used consistently) and a tens machine which also helps.
I just thought it was something I had to manage from now on.
Well, I had a hysterectomy last week due to fibroid. It was enlarged uterus. My doctor said I would probably feel better in many ways. I looked up sciatica/ uterus/ fibroids and suddenly found out that might have been the cause of my pain. I have not had any pain in my sciatica since surgery. I even sat in a chair for 3 hours last week and no symptoms. This is life changing. No one ever even hinted it could be connected to gynecological issues. I feel I have been unexpectedly been given my life back. I want to shout it from the roof tops.