Visceral Manipulation™ can help in cases of gastroparesis. Gastroparesis is delayed gastric emptying leaving food in the stomach longer than normal. Many people refer to the stomach as the belly in general. Whenever I say stomach, I’m referring to the actual stomach organ.
Symptoms of gastroparesis may include:
- nausea
- vomiting typically two hours after eating and may contain food particles that weren’t broken down. Although the vomiting can occur at other times. However, vomiting isn’t present with everyone with gastroparesis.
- early satiety
- pressure under the ribcage
- abdominal bloating
- pain can vary depending on the severity of gastroparesis and can be quite debilitating
- lack of appetite
- GERD When food sits in the stomach longer than it should it starts to ferment creating pressure on the lower esophageal sphincter. This pressure can lead to sphincter dysfunction allowing for acid reflux.
- malnutrition and weight loss in extreme cases
Causes:
- damage to the vagus nerve during surgery
- impairment of the vagus nerve
- infections, tumors, seizures
- diabetes mellitus (which is the #1 cause)
- hyperglycemia delays stomach emptying
- diseases that cause damage to the stomach muscles such as scleroderma
- dysfunction of the nervous system reflexes
- certain medications such as narcotics and anticholinergics. Makes me wonder if the rise of gastroparesis diagnosis correlates with the opioid epidemic.
- hypothyroidism
- metabolic disorders
- mineral imbalances
- most often a cause cannot be found and therefore is referred to as idiopathic
- Pylorus dysfunction – “recent studies suggest that loss of pyloric distensibility could cause a functional obstruction” (source) The pylorus is the area of the stomach that opens into the first part of the small intestine. So, if it’s not functioning well, it would make it difficult for the stomach to empty. In my experience, Visceral Manipulation™ works well to restore the function of the pylorus.
- Other causes
Talk to your doctor about confirming a diagnosis. Keep in mind that…”Gastroparesis is often inaccurately defined and misdiagnosed in patients whose symptoms have little to do with the rate at which the stomach empties its contents. A minority of patients with severely impaired gastric motor functions do have an inability of the stomach to empty, resulting in vomiting, weight loss, bezoars, and, in patients with diabetes, impairment of diabetic control; however, the majority of patients are mislabeled as gastroparesis. The temptation to rush to tests and the subsequent misdiagnosis deflect attention from gathering critical elements of the patient’s history that may reveal other diagnoses (eg, rumination, dumping syndrome, cyclic vomiting syndrome, iatrogenic or central nausea) that may be more relevant and amenable to therapy.” (source)
As an abdominal therapist specializing in Visceral Manipulation™, I have worked with people who have been diagnosed with mild to moderate cases of gastroparesis. The following suggestions are what I have found extremely helpful for my clients. Of course, conventional medicine may offer other therapies such as pharmaceuticals or surgery, especially for severe cases.
What to do to help your stomach out:
- address any underlying causes. If you are taking a medication that negatively affects the stomach, talk to your doctor about an alternative. For instance, if your foot hurts because you have a rock in your shoe, take the rock out instead of spending a bunch of money on treatments.
If hypothyroidism, diabetes, or other underlying cause is revealed please work with a qualified physician. By the way, lad test results may be read differently from physician to physician. What an MD defines as “normal” may not be optimal according to ND. The types of thyroid tests ordered are usually more comprehensive when done by a naturopathic physician. - talk to a functional nutritionist or ND about diet. Some foods are more difficult to digest (unfortunately, fiber slows stomach emptying) so you want to reduce the burden on your stomach while making sure you are taking inadequate nutrition including minerals.
- warm softer meals are easier to digest than cold high fiber meals.
- eat smaller meals. The stomach works better when it’s not full.
- eat your meals in a relaxed atmosphere. Don’t talk about politics during meals. Anxiety and fear can slow digestion by up to 36 hours!
- Avoid cold beverages with meals!
- Ginger accelerates gastric emptying and stimulates antral contractions in healthy volunteers. (Source)
- There are no teeth in your stomach! Chew your food well. Each stage of digestion only works as the stage that came before. When you chew your food well the digestive enzymes can actually reach the fine particles to break them down.
- Digestion starts in the brain before you ever put food in your mouth. Smelling your food to stimulate the digestive juices will prepare the stomach for the incoming well-chewed food.
- Avoid laying down after for 4-5 hours after a meal. In fact, go for a relaxing walk after meals. this will help with emptying the stomach through gravity and stimulate the stomach and spleen meridians that run through the legs.
- Do vagal nerve stimulating exercises.
- Visceral Manipulation™ aims to help the body restore its natural motility and mobility. Mobility is movement from external sources such as breathing, massage, and full-body movement. Motility is an intrinsic (contained wholly within the organ) movement that all organs have (see chart below).
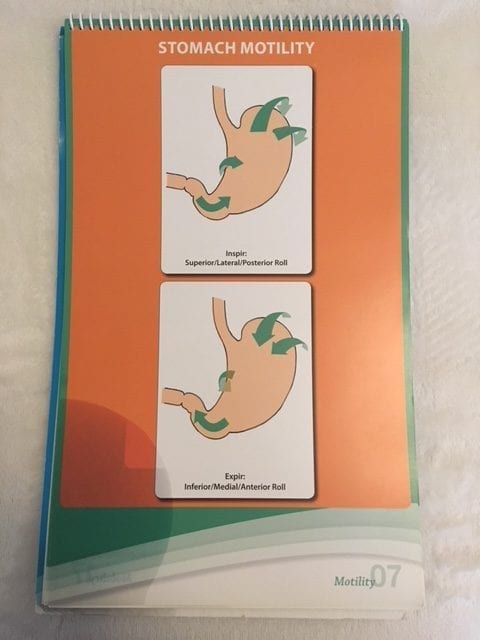
Visceral Mobility and Motility Chart by Jean Pierre Barral DO
Finding a Visceral Manipulation™ practitioner:
I offer Visceral Manipulation™ in the Ludington, Michigan area as well as other abdominal therapies. Visit my Nurturance website.
You can also search for a Visceral Manipulation™ practitioner by area on the Barral Institute website.
Effects of ginger on gastric emptying and motility in healthy humans European Journal of Gastroenterology & Hepatology: May 2008 – Volume 20 – Issue 5 – p 436-440 doi: 10.1097/MEG.0b013e3282f4b224
Original Articles: Gastric Motility
A Critical Review of the Current Clinical Landscape of Gastroparesis